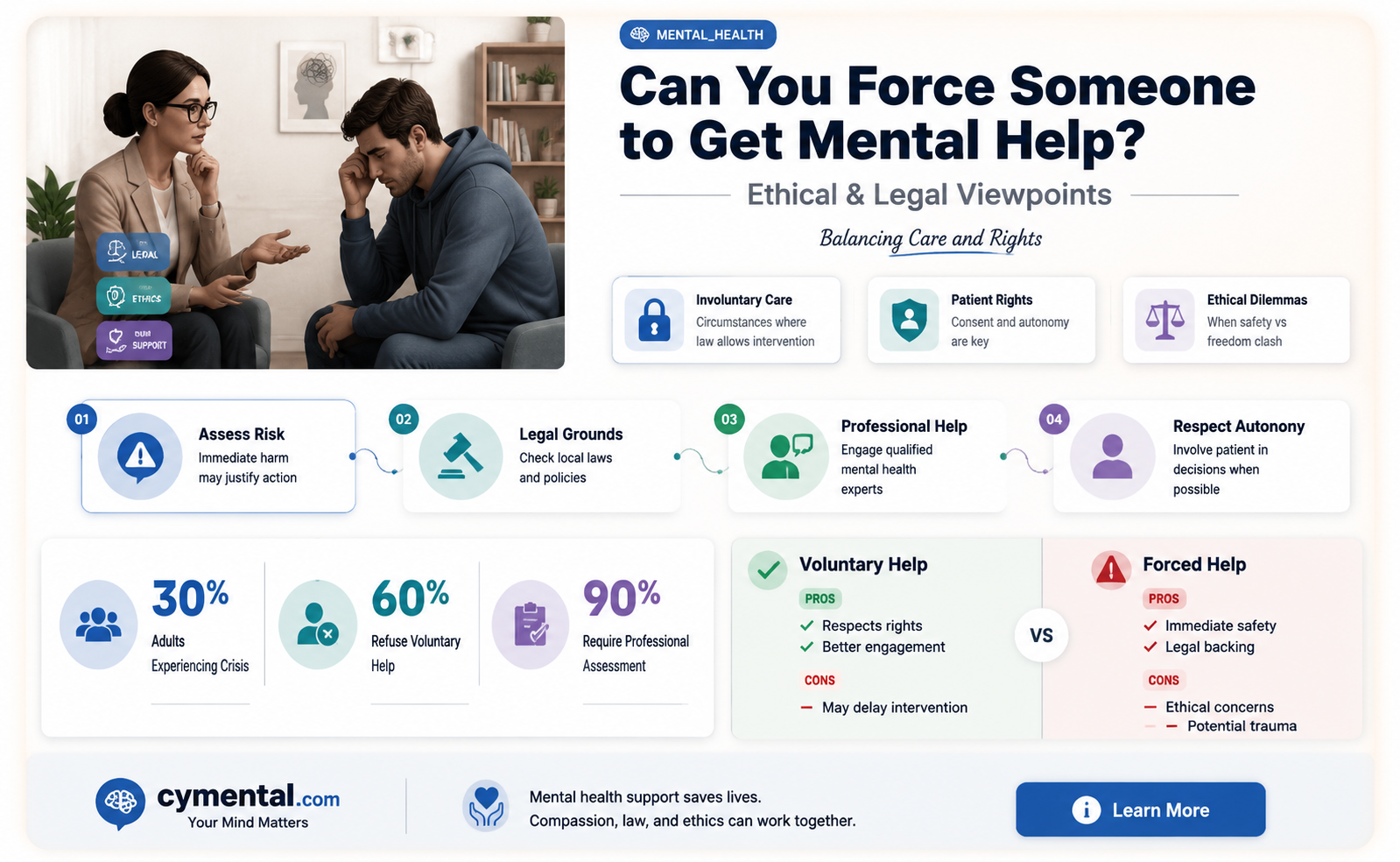
The question of whether you can force someone to get mental health treatment is complex and ethically charged, touching on issues of autonomy, human rights, and public safety. While it’s natural to want to help a loved one struggling with mental illness, involuntary treatment is typically a last resort and varies widely by jurisdiction. Laws like involuntary commitment or court-ordered treatment exist in many places but are strictly regulated to balance the individual’s rights with the need for care. Factors such as the person’s capacity to make decisions, the severity of their condition, and the risk they pose to themselves or others often determine whether intervention is legally and ethically justified. Ultimately, the goal is to provide support while respecting dignity and fostering trust, as coercion can strain relationships and undermine long-term recovery.
Explore related products

$20.49 $36.99





What You'll Learn
![]()
Legal requirements for involuntary commitment
Involuntary commitment, the legal process of compelling an individual to receive mental health treatment against their will, is a complex and highly regulated procedure. It is not a decision taken lightly, as it involves a delicate balance between protecting the individual's rights and ensuring public safety. The legal requirements for such an intervention vary across jurisdictions, but they generally follow a stringent set of criteria to safeguard against abuse.
The Legal Threshold: A High Bar to Clear
The legal system typically sets a high threshold for involuntary commitment, requiring clear and convincing evidence that an individual poses a significant risk to themselves or others due to a mental health condition. This standard is intentionally rigorous to prevent arbitrary detentions and protect civil liberties. For instance, in the United States, the criteria often include a determination that the person is unable to make informed decisions about their treatment and that their condition is likely to deteriorate without intervention. This assessment must be made by qualified mental health professionals, ensuring a level of expertise in the decision-making process.
A Step-by-Step Process
- Petition and Evaluation: The process usually begins with a petition filed by a concerned party, such as a family member, healthcare professional, or law enforcement officer. This triggers an evaluation by a mental health professional who assesses the individual's condition and the potential risks. The evaluator must consider factors like the person's ability to understand their situation, the presence of suicidal or homicidal tendencies, and the likelihood of self-neglect.
- Legal Hearing: If the initial evaluation supports the need for involuntary commitment, a legal hearing is typically required. Here, a judge or magistrate examines the evidence, including expert testimony, to determine if the legal criteria are met. This step ensures an independent review, safeguarding against potential biases or errors in the initial assessment.
- Least Restrictive Alternative: A key principle in many legal systems is the concept of the "least restrictive alternative." This means that even if a person meets the criteria for involuntary commitment, the court must consider if less restrictive options, such as outpatient treatment or voluntary admission, could effectively address the concerns. This principle respects the individual's autonomy while still providing necessary care.
Challenges and Ethical Considerations
Involuntary commitment raises ethical dilemmas, particularly regarding personal freedom and the potential for misuse. Critics argue that it can lead to the stigmatization of individuals with mental health issues and may deter people from seeking help voluntarily. Moreover, cultural and socioeconomic factors can influence the interpretation of risk, potentially leading to disparities in how the law is applied. For instance, certain behaviors might be perceived as more threatening in specific cultural contexts, impacting the likelihood of involuntary commitment.
Practical Implications and Support
For those considering this route, it's crucial to understand the specific laws in your jurisdiction. Each country and, often, each state or region, has its own mental health act or legislation outlining the process. These laws detail the rights of individuals, the roles of various professionals, and the steps for appeal or review. Support services and advocacy groups can provide valuable guidance, ensuring that the process is navigated with sensitivity and adherence to legal requirements.
In summary, while involuntary commitment is a legal avenue to ensure mental health treatment, it is a measure of last resort, surrounded by rigorous safeguards. The process demands a careful, evidence-based approach, respecting individual rights while addressing critical mental health needs.
Supporting Mental Health: Effective Ways to Help a Loved One in Need
You may want to see also
Explore related products






![]()
Ethical concerns in forcing mental health treatment
Forcing someone into mental health treatment raises profound ethical dilemmas, particularly around autonomy versus protection. The principle of informed consent is a cornerstone of medical ethics, yet in cases of severe mental illness, individuals may lack the capacity to make rational decisions. This conflict pits the right to self-determination against the duty to prevent harm, either to the individual or others. For instance, involuntary commitment laws in many jurisdictions allow for temporary detention if a person poses an imminent risk, but this power must be wielded with extreme caution to avoid abuse.
Consider the case of a 28-year-old with untreated schizophrenia who refuses medication due to anosognosia, a condition where they cannot recognize their illness. Forcing treatment might stabilize their symptoms, but it also undermines their agency. Ethical practice requires a nuanced approach: assessing capacity through structured tools like the MacArthur Competence Assessment Tool, exploring less restrictive alternatives (e.g., outpatient treatment orders), and ensuring regular judicial review of involuntary measures. Balancing care and coercion demands constant vigilance to respect human dignity.
From a persuasive standpoint, proponents of involuntary treatment argue it serves as a lifeline for those unable to seek help independently. Studies show that involuntary patients often report improved quality of life post-treatment, though this data is contentious. Critics counter that such interventions can erode trust in the mental health system, particularly among marginalized groups with historical trauma. For example, Black individuals in the U.S. are disproportionately subjected to involuntary commitment, reflecting systemic biases. Ethical frameworks must address these disparities by prioritizing cultural competence and equitable access to voluntary services.
A comparative analysis reveals varying global approaches. In countries like Sweden, involuntary treatment is rare, with emphasis on community-based support and advance directives. Contrastingly, the U.S. relies heavily on involuntary hospitalization, often due to gaps in preventive care. This disparity highlights the role of societal infrastructure in shaping ethical outcomes. Investing in early intervention programs, such as youth mental health teams or peer support networks, could reduce the need for coercive measures while upholding individual rights.
Practically, clinicians face the challenge of implementing ethical involuntary treatment. Key steps include: documenting clear evidence of risk, involving family or advocates in decision-making, and using the least restrictive interventions (e.g., oral medications over long-acting injectables). Cautions include avoiding overreliance on coercion, monitoring for adverse effects (e.g., akathisia from antipsychotics), and ensuring follow-up care to prevent relapse. Ultimately, ethical involuntary treatment is not about control but about creating a pathway to recovery that respects the person’s humanity.
Supporting Reluctant Loved Ones: Strategies for Accessing Mental Health Care
You may want to see also
Explore related products






![]()
Criteria for emergency psychiatric holds
In the United States, emergency psychiatric holds, often referred to as involuntary commitment or emergency hospitalization, are governed by specific criteria designed to balance individual rights with public safety. These holds typically last 72 hours, during which a mental health evaluation is conducted to determine the need for further treatment. The primary criterion across most states is the presence of an imminent risk of harm to oneself or others due to a mental health condition. This risk must be substantiated by observable behaviors, such as suicidal threats, homicidal ideation, or severe self-neglect, rather than mere speculation.
To initiate an emergency psychiatric hold, a qualified professional—often a physician, psychologist, or law enforcement officer—must file a petition or make a formal declaration. In California, for instance, the Lanterman-Petris-Short (LPS) Act requires that two professionals or a professional and a law enforcement officer concur on the need for detention. In contrast, New York’s criteria under its Mental Hygiene Law allow a single physician to authorize a hold if the individual meets the danger threshold. These variations highlight the importance of understanding state-specific laws when navigating involuntary commitment.
A critical aspect of these holds is the requirement for a prompt evaluation by a mental health professional. During the 72-hour period, the individual must be assessed to determine if they meet the legal standard for continued involuntary treatment. This evaluation includes a review of medical history, current symptoms, and the likelihood of decompensation without intervention. For example, a person with untreated schizophrenia exhibiting severe psychosis and an inability to care for themselves might be deemed a candidate for extended care. However, the bar for long-term commitment is significantly higher, often requiring judicial approval and clear evidence of ongoing danger.
While emergency psychiatric holds are a necessary tool for crisis intervention, they are not without ethical and practical challenges. Critics argue that such measures can infringe on civil liberties, particularly when applied inconsistently or without sufficient oversight. To mitigate these concerns, many states require regular reviews of the individual’s condition and mandate the least restrictive treatment options. For families or caregivers seeking to support a loved one, understanding these criteria and processes is essential. Practical tips include documenting concerning behaviors, familiarizing oneself with local resources, and consulting legal or mental health professionals for guidance.
In conclusion, emergency psychiatric holds serve as a critical mechanism for addressing acute mental health crises, but their application is tightly regulated to protect individual rights. By understanding the specific criteria, legal procedures, and ethical considerations, stakeholders can navigate this complex system more effectively. Whether you are a concerned family member, a healthcare provider, or a policymaker, awareness of these guidelines ensures that involuntary commitment is used judiciously and compassionately.
Supporting Your Adult Son’s Mental Health: Practical Steps for Parents
You may want to see also
Explore related products





![]()
Role of family in intervention decisions
Family members often find themselves at a crossroads when a loved one struggles with mental health issues but resists seeking help. The decision to intervene is complex, balancing respect for autonomy with the urgency of ensuring safety and well-being. In many jurisdictions, involuntary commitment laws allow for forced treatment under specific conditions, but the family’s role in initiating and navigating this process is critical. They are often the first to recognize distressing symptoms—such as severe depression, psychosis, or suicidal ideation—and their observations can provide essential context for mental health professionals assessing the need for intervention.
Consider the steps a family might take when faced with this dilemma. First, educate yourself about the legal criteria for involuntary treatment in your area. For instance, in the U.S., most states require proof that the individual is a danger to themselves or others, or unable to care for their basic needs. Document specific incidents that demonstrate this risk, such as self-harm attempts or neglect of personal hygiene. Second, consult a mental health professional who can guide the process, possibly through a formal mental health evaluation. Third, prepare for emotional resistance; the individual may feel betrayed or angry, so approach the conversation with empathy, emphasizing concern rather than control.
However, not all interventions involve legal force. Families can play a pivotal role in encouraging voluntary treatment through supportive strategies. For example, staging a structured family meeting—often referred to as a "soft intervention"—can create a safe space for open dialogue. Use "I" statements to express feelings without assigning blame, such as, "I feel worried when I see you struggling, and I want to help." Offer concrete resources, like the contact information for a therapist or a list of local support groups. For younger individuals (under 18), parental consent can facilitate quicker access to treatment, though this should still involve the child’s input to foster cooperation.
The ethical considerations here cannot be overstated. Forcing someone into treatment can strain relationships and may undermine trust, particularly if the individual perceives it as coercive. Families must weigh the immediate risks against the long-term impact on the individual’s autonomy and dignity. In cases of severe mental illness, such as schizophrenia or bipolar disorder, where insight into the condition is limited, involuntary treatment might be necessary to stabilize the individual before exploring voluntary options. Yet, even in these scenarios, involving the person in decision-making as much as possible can mitigate feelings of powerlessness.
Ultimately, the family’s role in intervention decisions is both powerful and delicate. They serve as advocates, educators, and emotional anchors, but their actions must be informed, compassionate, and legally sound. By understanding the limits of their influence and collaborating with professionals, families can navigate this challenging terrain in a way that prioritizes both recovery and respect for the individual’s humanity.
Music's Power: Boosting Middle Schoolers' Mental Health and Well-Being
You may want to see also
Explore related products






![]()
Effectiveness of coerced mental health care
Coercion in mental health care often hinges on legal frameworks like involuntary commitment or court-mandated treatment, but its effectiveness remains a contentious issue. Studies show that forced treatment can stabilize acute symptoms in conditions like schizophrenia or severe bipolar disorder, particularly when paired with antipsychotic medications such as olanzapine (10–20 mg/day) or haloperidol (5–10 mg/day). However, these gains are often short-term, with relapse rates climbing once coercion ends. For instance, a 2014 meta-analysis in *The Lancet* found that 70% of involuntarily treated patients discontinued medication within a year of discharge, highlighting the limitations of coercion as a standalone solution.
The psychological impact of coerced care complicates its effectiveness. Patients subjected to forced treatment frequently report feelings of resentment, loss of autonomy, and diminished trust in healthcare providers. This erosion of therapeutic alliance can undermine long-term engagement with mental health services. For example, a 2019 study in *Psychiatric Services* revealed that individuals who experienced coercion were 30% less likely to voluntarily seek follow-up care compared to those treated consensually. Such findings suggest that while coercion may address immediate safety concerns, it risks alienating patients from the very systems designed to support them.
A comparative analysis of coerced versus voluntary treatment models reveals stark differences in outcomes. Voluntary programs, such as Assertive Community Treatment (ACT) or peer-supported recovery, often yield higher adherence rates and better quality of life metrics. ACT teams, which provide intensive, personalized care in community settings, have been shown to reduce hospitalization rates by up to 50% among participants. In contrast, coerced treatment tends to focus on symptom suppression rather than holistic recovery, neglecting critical factors like social support and personal agency. This disparity underscores the importance of prioritizing patient-centered approaches even in crisis situations.
Practical considerations further challenge the effectiveness of coerced care. Implementing involuntary treatment requires significant resources, including legal proceedings, specialized facilities, and trained personnel. These demands can strain already overburdened mental health systems, diverting attention from preventive and early intervention efforts. For instance, in the U.S., the average cost of a 30-day involuntary hospitalization exceeds $30,000, compared to $5,000 for outpatient ACT services. Such financial disparities raise ethical questions about resource allocation and the sustainability of coercive practices.
Ultimately, the effectiveness of coerced mental health care is a delicate balance between crisis management and long-term recovery. While it may serve as a necessary intervention in life-threatening situations, its success hinges on integrating it into a broader, voluntary care framework. Clinicians and policymakers must navigate this tension by emphasizing informed consent, minimizing coercion, and fostering environments where patients feel empowered to participate in their treatment. Without such measures, coerced care risks becoming a Band-Aid solution that fails to address the root causes of mental illness.
Helping Reluctant Loved Ones Access Mental Health Care in Texas
You may want to see also
Frequently asked questions
In most cases, you cannot force someone to get mental health treatment unless they pose an immediate danger to themselves or others, and even then, legal procedures must be followed, such as involuntary commitment.
You can encourage them to seek help, offer support, and involve a mental health professional or crisis intervention team if there’s an immediate risk. However, you cannot force treatment without legal intervention.
Involuntary commitment is a last resort and requires meeting strict legal criteria, such as the person being a danger to themselves or others and unable to care for themselves. It is not a common or easy process.
Family members cannot force treatment on their own. They can petition the court for involuntary commitment if the person meets legal criteria, but the decision ultimately lies with a judge or mental health professional.
Alternatives include open communication, offering support, involving a therapist or counselor, and using crisis hotlines or intervention services. Building trust and understanding can often encourage voluntary treatment.