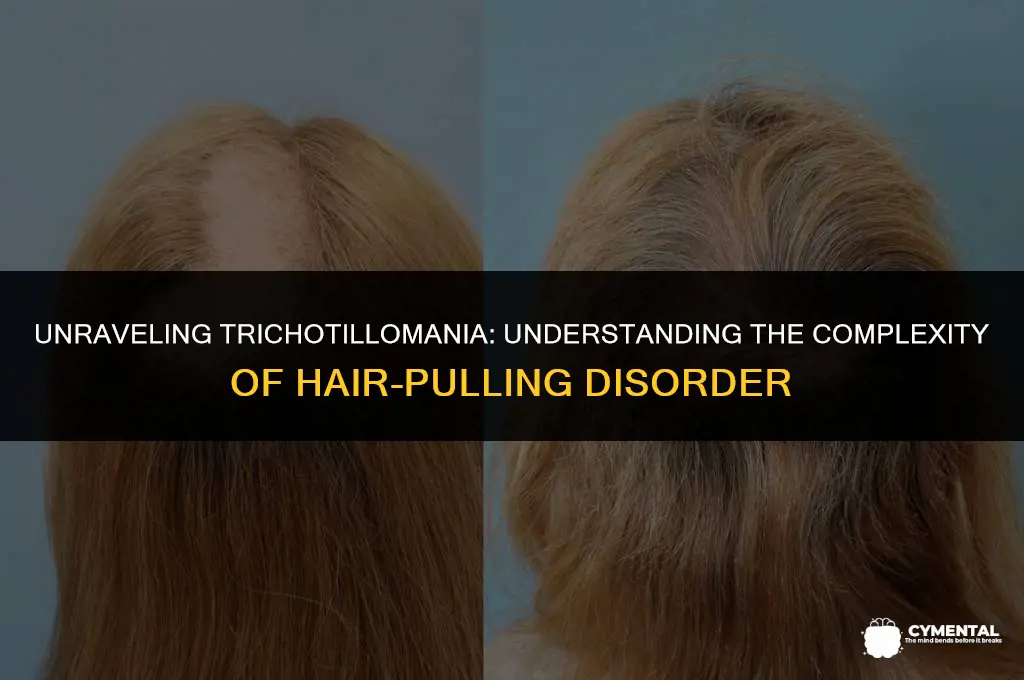
Trichotillomania, often referred to as hair-pulling disorder, is a complex condition characterized by the irresistible urge to pull out one's hair, leading to noticeable hair loss and even bald patches. While it may seem like a behavioral issue, trichotillomania is recognized as a mental health disorder, specifically classified as an obsessive-compulsive related disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). This classification underscores the psychological distress and impairment in daily functioning that individuals with trichotillomania often experience. The disorder can affect people of all ages and genders, though it tends to onset in childhood or adolescence and can persist into adulthood if left untreated. Understanding trichotillomania as a mental health condition is crucial for providing appropriate support and treatment to those affected.
| Characteristics | Values |
|---|---|
| Definition | Trichotillomania is a mental disorder characterized by a recurrent and irresistible urge to pull out one's hair, leading to noticeable hair loss and even bald patches. |
| Classification | It is classified as an obsessive-compulsive related disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). |
| Prevalence | It is estimated to affect approximately 2-3% of the global population, with higher rates in females. |
| Age of Onset | Trichotillomania typically begins in childhood or adolescence, but it can also start in adulthood. |
| Symptoms | Symptoms include repetitive hair pulling, resulting in hair loss, and often accompanied by feelings of shame, embarrassment, or distress. |
| Causes | The exact cause is unknown, but it is believed to be related to genetic, environmental, and psychological factors. |
| Risk Factors | Risk factors include family history of the disorder, stress, anxiety, and other mental health conditions. |
| Diagnosis | Diagnosis is based on clinical evaluation, patient history, and the presence of characteristic symptoms. |
| Treatment | Treatment options include cognitive-behavioral therapy (CBT), medication, and behavioral interventions such as habit reversal training. |
| Prognosis | With proper treatment, many individuals with trichotillomania can experience significant improvement in symptoms and quality of life. |
| Comorbidities | Trichotillomania often co-occurs with other mental health disorders, such as anxiety, depression, and obsessive-compulsive disorder. |
| Impact on Daily Life | The disorder can significantly impact daily life, causing social withdrawal, decreased self-esteem, and difficulties in personal and professional relationships. |
| Support Groups | There are various support groups and online communities available for individuals with trichotillomania and their families. |
| Research | Ongoing research is focused on understanding the underlying causes of trichotillomania and developing more effective treatment strategies. |
| Awareness | Raising awareness about trichotillomania is crucial to reduce stigma and encourage individuals to seek help. |
Explore related products






What You'll Learn
![]()
Definition and Diagnosis
Trichotillomania is characterized by the recurrent and irresistible urge to pull out one's hair, leading to noticeable hair loss and even bald patches. This behavior is often accompanied by a sense of relief or gratification, followed by feelings of guilt or shame. To diagnose trichotillomania, mental health professionals look for specific criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). These criteria include the presence of hair pulling resulting in hair loss, repeated attempts to decrease or stop the behavior, and significant distress or impairment in social, occupational, or other areas of functioning.
The diagnostic process typically involves a thorough clinical interview, during which the individual's medical and psychiatric history is reviewed. The clinician may also ask about the frequency and severity of hair pulling, as well as any associated emotions or triggers. In some cases, a physical examination may be conducted to assess the extent of hair loss and rule out other potential causes. Additionally, psychological assessments or questionnaires may be used to evaluate the individual's mental health and identify any co-occurring conditions, such as anxiety or depression.
It is important to note that trichotillomania can be difficult to diagnose, as individuals may be reluctant to disclose their hair pulling behavior due to feelings of shame or embarrassment. Furthermore, the disorder can mimic other conditions, such as alopecia or hair loss due to medical treatments. Therefore, a comprehensive and empathetic approach is essential in accurately diagnosing and treating trichotillomania. Mental health professionals must create a safe and non-judgmental environment, encouraging open communication and understanding.
Once diagnosed, trichotillomania can be treated using a combination of behavioral therapies, such as cognitive-behavioral therapy (CBT) and habit reversal training (HRT), as well as medications like selective serotonin reuptake inhibitors (SSRIs). These interventions aim to address the underlying causes of the disorder, reduce hair pulling behavior, and improve overall quality of life. With proper treatment and support, individuals with trichotillomania can learn to manage their symptoms and regain control over their lives.
Understanding Gender Dysphoria: A Complex Exploration Beyond Labels
You may want to see also
Explore related products






![]()
Symptoms and Behaviors
Trichotillomania, a body-focused repetitive behavior, is characterized by the irresistible urge to pull out one's hair, leading to noticeable hair loss and even bald patches. This disorder often begins in childhood or adolescence and can persist into adulthood if left untreated. Individuals with trichotillomania may experience a range of emotions, from shame and embarrassment to relief and pleasure, when engaging in hair-pulling behaviors.
The symptoms of trichotillomania can vary in severity and presentation. Some individuals may experience episodic hair-pulling, while others may engage in this behavior chronically. The disorder can affect any area of the body where hair is present, but the most common sites include the scalp, eyebrows, and eyelashes. In severe cases, hair-pulling can lead to significant hair loss, scarring, and even infection.
Trichotillomania is often associated with other mental health conditions, such as anxiety, depression, and obsessive-compulsive disorder. Individuals with trichotillomania may also experience difficulties in social and occupational settings due to the visible effects of hair-pulling. Treatment for trichotillomania typically involves a combination of behavioral therapy, medication, and support groups. Cognitive-behavioral therapy, in particular, has been shown to be effective in reducing hair-pulling behaviors and improving overall functioning.
It is essential to recognize trichotillomania as a legitimate mental health disorder rather than a mere habit or personal quirk. Early identification and intervention can significantly improve outcomes for individuals struggling with this condition. By increasing awareness and understanding of trichotillomania, we can help reduce the stigma associated with this disorder and encourage those affected to seek the help they need.
Exploring the Possibilities: Can Mental Disorders Be Cured?
You may want to see also
Explore related products






![]()
Causes and Risk Factors
Trichotillomania, a disorder characterized by the irresistible urge to pull out one's hair, leading to noticeable hair loss, is indeed classified as a mental disorder. It falls under the category of obsessive-compulsive and related disorders in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The exact causes of trichotillomania are not fully understood, but research suggests a combination of genetic, environmental, and neurological factors contribute to its development.
Genetically, trichotillomania tends to run in families, indicating a possible hereditary component. Studies have identified several genes that may be involved in the disorder, including those related to dopamine and serotonin, neurotransmitters that play a role in mood regulation and impulse control. Environmental factors, such as childhood trauma, stress, and social isolation, can also trigger or exacerbate trichotillomania. Individuals who have experienced abuse, neglect, or bullying may be more likely to develop the disorder as a coping mechanism.
Neurologically, trichotillomania is associated with abnormalities in brain structure and function. Functional magnetic resonance imaging (fMRI) studies have shown differences in brain activity patterns between individuals with trichotillomania and those without the disorder. These differences are particularly evident in regions of the brain involved in impulse control, emotion regulation, and reward processing. Additionally, trichotillomania often co-occurs with other mental health conditions, such as anxiety, depression, and obsessive-compulsive disorder (OCD), further supporting its classification as a mental disorder.
Risk factors for trichotillomania include a family history of the disorder, personal history of trauma or abuse, and the presence of other mental health conditions. Children and adolescents are at higher risk, with the disorder typically beginning during these developmental stages. Females are also more likely to develop trichotillomania than males, although the reasons for this gender disparity are not yet fully understood.
In conclusion, trichotillomania is a complex mental disorder with multiple contributing factors. While the exact causes remain unclear, research has identified genetic, environmental, and neurological elements that play a role in its development. Understanding these factors is crucial for developing effective treatment strategies and providing support for individuals affected by the disorder.
Exploring Canine Mental Health: Do Dogs Experience Disorders?
You may want to see also
Explore related products





![]()
Treatment Options
Trichotillomania, a disorder characterized by the irresistible urge to pull out one's hair, can be treated through various therapeutic approaches. Cognitive-behavioral therapy (CBT) is often the first line of treatment, helping individuals identify and change negative thought patterns and behaviors associated with hair pulling. Another effective method is habit reversal training (HRT), which teaches individuals to recognize the urge to pull and replace it with a less harmful behavior.
Medications can also play a role in managing trichotillomania. Selective serotonin reuptake inhibitors (SSRIs) are commonly prescribed to help reduce the compulsive behavior associated with the disorder. In some cases, other medications such as mood stabilizers or antipsychotics may be used to address co-occurring conditions or symptoms.
For those who do not respond well to traditional treatments, alternative therapies may be considered. These can include mindfulness-based interventions, which help individuals develop greater awareness of their thoughts and actions, and acceptance and commitment therapy (ACT), which focuses on helping individuals accept their experiences and take action towards valued life goals.
In addition to these formal treatments, there are several self-help strategies that individuals with trichotillomania can employ. These may include keeping a journal to track hair-pulling episodes, using relaxation techniques such as deep breathing or meditation, and engaging in activities that promote a sense of accomplishment and self-worth.
It is important to note that treatment for trichotillomania should be tailored to the individual's specific needs and circumstances. A combination of therapies may be necessary to achieve the best results, and ongoing support and monitoring are often essential to maintaining progress and preventing relapse.
Understanding Intellectual Disabilities: A Comprehensive Overview
You may want to see also
Explore related products





![]()
Prognosis and Outlook
Trichotillomania, a body-focused repetitive behavior disorder, presents a complex prognosis and outlook for those affected. While some individuals may experience periods of remission, others may struggle with the condition chronically. The disorder often begins in childhood or adolescence and can persist into adulthood if left untreated. Early intervention is crucial in improving the long-term outlook for individuals with trichotillomania.
Treatment approaches, such as cognitive-behavioral therapy (CBT) and medication, can be effective in managing symptoms and promoting recovery. However, the prognosis varies widely among individuals, with some responding well to treatment while others may not. Factors such as the severity of the disorder, the presence of co-occurring mental health conditions, and the individual's motivation to change can all impact the outlook.
In addition to professional treatment, self-help strategies and support groups can play a valuable role in managing trichotillomania. Individuals can benefit from learning stress management techniques, developing healthier coping mechanisms, and connecting with others who understand their struggles. With the right combination of treatment and support, many individuals with trichotillomania can lead fulfilling lives and achieve significant improvement in their symptoms.
It is important to note that trichotillomania is not a reflection of personal weakness or a lack of willpower. Rather, it is a legitimate mental health condition that requires understanding, compassion, and appropriate treatment. By raising awareness and reducing stigma, we can help individuals with trichotillomania seek the help they need and improve their overall prognosis and outlook.
Exploring the Complex Relationship Between Religion and Mental Health
You may want to see also
Frequently asked questions
Yes, trichotillomania is classified as a mental disorder. It is characterized by the irresistible urge to pull out one's hair, leading to noticeable hair loss and often causing distress or impairment in social, occupational, or other areas of functioning.
The common symptoms of trichotillomania include the repetitive and compulsive urge to pull out hair from the scalp, eyebrows, eyelashes, or other areas of the body. This behavior often results in noticeable hair loss, and individuals may experience a sense of relief or gratification when pulling out their hair, followed by feelings of guilt or shame.
Trichotillomania is diagnosed through a combination of clinical evaluation and diagnostic criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). A healthcare professional will assess the individual's symptoms, behavior, and medical history to determine if the criteria for trichotillomania are met.
The exact causes of trichotillomania are not fully understood, but it is believed to be a complex interplay of genetic, environmental, and psychological factors. Some potential triggers may include stress, anxiety, depression, or other mental health conditions. Additionally, certain personality traits or compulsive behaviors may contribute to the development of trichotillomania.
Treatment for trichotillomania typically involves a combination of behavioral therapy, cognitive-behavioral therapy (CBT), and sometimes medication. Behavioral therapy may include habit reversal training or other techniques to help individuals recognize and resist the urge to pull out their hair. CBT can help address underlying thoughts and beliefs that contribute to the behavior. Medications such as selective serotonin reuptake inhibitors (SSRIs) may also be prescribed to help manage symptoms.