The question of whether there should be free mental health services for police officers is a critical and timely issue, given the unique and often traumatic experiences they face in their line of duty. Police officers are routinely exposed to high-stress situations, violence, and human suffering, which can take a significant toll on their mental well-being. Despite this, many officers hesitate to seek help due to stigma, fear of career repercussions, or financial barriers. Providing free mental health support tailored to their needs could not only improve individual officers' quality of life but also enhance their ability to serve the public effectively. It raises important discussions about workplace responsibility, societal support for first responders, and the long-term benefits of prioritizing mental health in high-risk professions.
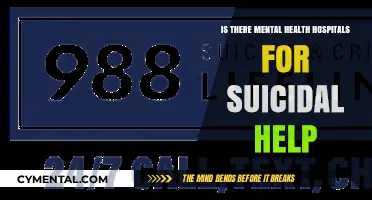
| Characteristics | Values |
|---|---|
| Prevalence of Mental Health Issues | High rates of PTSD, depression, anxiety, and burnout among police officers |
| Barriers to Accessing Help | Stigma, fear of career repercussions, lack of affordable resources |
| Impact on Job Performance | Mental health issues can impair decision-making and increase errors |
| Public Safety Concerns | Stressed officers may pose risks to themselves and the public |
| Cost-Effectiveness | Free mental health services can reduce long-term healthcare and legal costs |
| Officer Retention | Improved mental health support can increase job satisfaction and retention |
| Community Trust | Officers with better mental health may engage more positively with the public |
| Existing Programs | Some departments offer limited mental health resources, but coverage is inconsistent |
| Legislative Support | Growing advocacy for mandated mental health services for law enforcement |
| Stigma Reduction Efforts | Campaigns to normalize seeking mental health help within police culture |
| Data on Effectiveness | Studies show improved officer well-being and reduced absenteeism with support |
| Public Opinion | Majority support for free mental health services for police officers |
Explore related products

$19.95





What You'll Learn
- Funding Sources: Explore government budgets, public-private partnerships, and grants to sustain free mental health services
- Accessibility: Ensure 24/7 availability, confidential platforms, and diverse therapy options for all officers
- Stigma Reduction: Implement campaigns, training, and peer support to encourage officers to seek help
- Specialized Care: Provide trauma-informed therapists trained in police-specific stressors and critical incident responses
- Mandatory Check-Ins: Debate regular mental health screenings versus voluntary participation for officers' well-being
![]()
Funding Sources: Explore government budgets, public-private partnerships, and grants to sustain free mental health services
Government budgets often allocate funds to public safety, yet mental health services for police officers remain underfunded. Reallocating a fraction of existing law enforcement budgets—say, 5%—to mental health programs could provide immediate, sustainable support. For instance, a city with a $100 million police budget could redirect $5 million annually to fund counseling services, peer support programs, and crisis intervention training. This approach leverages current resources without requiring new taxes or fees, ensuring officers receive care without straining public finances.
Public-private partnerships offer another viable funding stream by combining government oversight with corporate investment. Companies could sponsor mental health initiatives in exchange for tax incentives or positive public relations. For example, a tech firm might fund a digital therapy platform for officers, while a healthcare provider could offer discounted services. Such partnerships not only reduce the financial burden on governments but also foster community engagement, creating a shared responsibility for officer well-being. However, clear guidelines must ensure private interests do not compromise service quality or accessibility.
Grants from federal, state, or philanthropic organizations provide targeted funding for innovative mental health programs. Police departments could apply for grants like the U.S. Department of Justice’s COPS Office initiatives or foundations focused on public health. A successful grant application might secure $250,000 to implement a 24/7 crisis hotline staffed by mental health professionals. While grants offer flexibility, they often require rigorous reporting and may not guarantee long-term funding, necessitating a diversified funding strategy to avoid service disruptions.
Combining these funding sources—government reallocation, public-private partnerships, and grants—creates a robust financial framework for free mental health services. For instance, a mid-sized police department could allocate $1 million from its budget, secure $500,000 through corporate sponsorship, and win a $300,000 grant, totaling $1.8 million annually. This multi-pronged approach ensures stability, scalability, and accountability, addressing the urgent need for officer mental health support while maximizing resource efficiency.
Finding Mental Health Support in North Carolina: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Accessibility: Ensure 24/7 availability, confidential platforms, and diverse therapy options for all officers
Police officers face unique stressors—high-stakes decisions, trauma exposure, and irregular shifts—that can erode mental resilience over time. Ensuring 24/7 access to mental health support isn’t just a perk; it’s a necessity. A crisis doesn’t adhere to a 9-to-5 schedule, and neither should the resources designed to address it. Implementing round-the-clock availability through hotlines, telehealth platforms, and on-site counselors can bridge the gap between an officer’s breaking point and the help they need. For instance, departments like the NYPD have introduced 24/7 peer support programs, proving that immediate access saves lives and fosters a culture of proactive care.
Confidentiality is the cornerstone of trust in mental health services, yet it remains a barrier for many officers. Fear of stigma or career repercussions often detaches them from seeking help. To dismantle this, departments must adopt encrypted, third-party platforms that guarantee anonymity. Apps like *First Responder Support Network* offer secure messaging and video sessions with therapists who specialize in law enforcement trauma. Pairing this with clear departmental policies that protect officers’ privacy—such as prohibiting access to therapy records by supervisors—can encourage utilization without fear of judgment or retaliation.
One size does not fit all in mental health care, especially for a workforce as diverse as law enforcement. Officers vary in age, cultural background, gender, and personal preferences, requiring a spectrum of therapy options. Cognitive Behavioral Therapy (CBT) might work for one officer, while another may benefit from mindfulness-based stress reduction or group therapy. Departments should partner with providers offering modalities like EMDR for trauma, couples counseling for relationship strain, or even pet therapy for emotional support. For example, the Los Angeles Police Department’s Wellness Program includes yoga, meditation, and art therapy, demonstrating how diverse options can cater to individual needs.
Practical implementation demands a multi-faceted approach. Start by auditing existing resources to identify gaps in accessibility, confidentiality, and diversity. Allocate funding for 24/7 services, ensuring at least one counselor is on call during night shifts. Train supervisors to recognize signs of distress and promote available resources without coercion. Finally, measure success through utilization rates and officer feedback, adjusting programs as needed. By treating mental health as an operational priority, departments can create a system where officers feel supported, not stigmatized, in seeking help.
Acting as Therapy: Unlocking Mental Health Benefits Through Performance
You may want to see also
Explore related products





![]()
Stigma Reduction: Implement campaigns, training, and peer support to encourage officers to seek help
Police officers face unique stressors—high-stakes decisions, trauma exposure, and public scrutiny—yet many hesitate to seek mental health support due to entrenched stigma. This reluctance exacerbates burnout, PTSD, and even suicidal ideation, compromising both officer well-being and public safety. Stigma reduction isn’t just a moral imperative; it’s a strategic necessity. Campaigns, training, and peer support must work in tandem to dismantle the culture of silence, replacing it with one that normalizes vulnerability as a sign of strength.
Consider the power of targeted campaigns. A study by the Ruderman Family Foundation found that 1 in 4 police officers has considered suicide, yet fewer than half seek help. Campaigns like the UK’s "Blue Light Programme" use relatable officer testimonials and data-driven messaging to challenge misconceptions about mental health. For instance, posters featuring officers saying, "Asking for help saved my career," paired with statistics on improved job performance post-therapy, can shift perceptions. Such campaigns should run annually, with measurable goals—e.g., a 20% increase in help-seeking behavior within 12 months—and be tailored to regional demographics and cultural nuances.
Training is equally critical. Officers often equate emotional resilience with professional competence, a belief reinforced by outdated academy curricula. Mandatory stigma-reduction training should be integrated into both recruit and in-service programs. For example, the "Beyond the Call" curriculum in Canada teaches officers to recognize mental health symptoms in themselves and peers, emphasizing that seeking help is a tactical decision, not a weakness. Trainers should use scenario-based exercises, such as role-playing how to respond to a colleague showing signs of distress, to build empathy and practical skills. Departments could also incentivize participation by offering continuing education credits or promotions tied to mental health advocacy.
Peer support programs provide the human element essential for breaking stigma. The NYPD’s "Peer Support Program" pairs officers with trained peers who have experienced similar challenges, fostering trust and confidentiality. These programs should be structured but flexible: weekly drop-in sessions, 24/7 hotlines, and anonymous digital platforms can cater to varying comfort levels. Peer supporters must receive at least 40 hours of initial training, covering active listening, crisis intervention, and referral protocols, with biannual refreshers to stay updated on best practices. Departments should also allocate dedicated funding for these programs, ensuring they aren’t viewed as optional add-ons but core components of officer wellness.
Combining these strategies creates a self-reinforcing system. Campaigns raise awareness, training builds skills, and peer support provides actionable pathways to care. For instance, after implementing a stigma-reduction initiative, the Seattle Police Department saw a 35% increase in officers accessing mental health services within two years. However, success requires leadership buy-in. Chiefs and commanders must publicly model help-seeking behavior, whether by sharing their own experiences or actively participating in training. Without visible commitment from the top, even the most well-designed programs risk being perceived as tokenistic.
In conclusion, stigma reduction isn’t a one-off initiative but a sustained cultural shift. By investing in campaigns, training, and peer support, departments can transform mental health care from a taboo into a tactical advantage. The question isn’t whether officers deserve free mental health support—it’s how quickly we can dismantle the barriers preventing them from accessing it.
Zumba's Mental Health Benefits: Dance Your Way to Wellness
You may want to see also
Explore related products






![]()
Specialized Care: Provide trauma-informed therapists trained in police-specific stressors and critical incident responses
Police officers face a unique set of stressors that can lead to significant mental health challenges. High-stakes decision-making, exposure to trauma, and the constant pressure to maintain public safety take a toll. While general mental health services are valuable, they often fall short in addressing the specific needs of law enforcement. This is where specialized care comes in.
Police officers require therapists trained in trauma-informed care who understand the nuances of police work. These therapists need to be equipped to handle the aftermath of critical incidents, such as shootings, fatalities, or domestic violence calls, which can leave lasting psychological scars.
Consider the following scenario: An officer witnesses a child's death in a car accident. A therapist unfamiliar with police realities might focus solely on grief processing. A trauma-informed therapist trained in police-specific stressors would recognize the officer's potential for guilt, self-doubt, and hypervigilance, tailoring treatment to address these unique reactions. This specialized approach ensures officers receive effective support, preventing long-term mental health issues like PTSD and burnout.
Implementing specialized care requires a multi-pronged approach. Firstly, departments should partner with mental health organizations to develop training programs specifically for therapists working with law enforcement. This training should cover topics like critical incident stress management, vicarious trauma, and the unique cultural dynamics within police departments. Secondly, departments need to actively encourage officers to seek help by fostering a culture of openness and destigmatizing mental health struggles. Confidentiality and accessibility are key; officers should have easy access to therapists who understand their world without fear of judgment or career repercussions.
The benefits of specialized care are clear. Officers who receive tailored support are better equipped to manage stress, make sound decisions, and maintain healthy relationships both on and off the job. This ultimately leads to a more resilient and effective police force, benefiting both officers and the communities they serve. Investing in specialized mental health care for police isn't just a matter of compassion; it's a strategic investment in public safety.
Ushering Hope: How Support Systems Aid Mental Health Recovery
You may want to see also
Explore related products


$19.95 $19.95



![]()
Mandatory Check-Ins: Debate regular mental health screenings versus voluntary participation for officers' well-being
Police officers face unique stressors—high-stakes decisions, trauma exposure, and public scrutiny—that can erode mental resilience over time. While free mental health resources are increasingly available, the question of whether participation should be mandatory or voluntary remains contentious. Mandatory check-ins could ensure early detection of issues like PTSD, depression, or burnout, potentially preventing crises. However, critics argue that forced screenings may stigmatize officers, discourage openness, or erode trust in the system. Striking the right balance requires examining both the benefits of proactive care and the risks of coercion in a profession built on autonomy and strength.
Consider the implementation of mandatory screenings as a structured, recurring process—for instance, biannual assessments using validated tools like the PTSD Checklist (PCL-5) or the Depression, Anxiety, and Stress Scale (DASS-21). These screenings could be paired with confidentiality guarantees and immediate access to resources, such as counseling or peer support groups. For example, the NYPD’s *Officer Resilience Program* integrates mandatory check-ins with voluntary follow-up care, demonstrating how structured intervention can coexist with personal agency. Such models prioritize early intervention while minimizing the perception of intrusion, addressing concerns about privacy and professionalism.
Voluntary participation, on the other hand, emphasizes individual choice and trust in officers’ self-awareness. This approach aligns with the culture of self-reliance often prevalent in law enforcement but carries risks. Without proactive outreach, officers may delay seeking help until symptoms become unmanageable. A 2021 study in *Police Practice and Research* found that only 30% of officers with probable PTSD sought treatment, often due to fear of judgment or career repercussions. Voluntary systems, while respectful of autonomy, may fail to address systemic barriers to care, leaving vulnerable officers unsupported.
A hybrid approach could bridge these gaps. For instance, mandatory initial screenings during onboarding and after critical incidents could establish a baseline, while subsequent check-ins remain voluntary. Departments could incentivize participation by framing screenings as part of professional development, not a sign of weakness. Practical steps include integrating mental health days into sick leave policies, offering anonymous reporting options, and training supervisors to recognize distress signals. By combining structure with flexibility, this model respects officers’ autonomy while fostering a culture of proactive well-being.
Ultimately, the debate between mandatory and voluntary check-ins reflects broader tensions in policing: accountability versus autonomy, prevention versus reaction. Mandatory screenings offer a safety net but risk alienating officers if not implemented thoughtfully. Voluntary systems preserve choice but may leave gaps in care. The ideal solution lies in tailoring approaches to departmental culture, leveraging data to refine strategies, and prioritizing trust-building. Whether through mandates or incentives, the goal remains the same: ensuring officers have the support they need to thrive in a demanding role.
Overcoming Mental Blocks: Strategies to Reclaim Focus and Creativity
You may want to see also
Frequently asked questions
Yes, free mental health services for police officers are essential due to the high-stress nature of their job, which often leads to trauma, burnout, and mental health issues like PTSD, anxiety, and depression.
Police officers face unique challenges, including exposure to violence, long hours, and societal scrutiny, which can take a significant toll on their mental well-being. Free support ensures they can access care without financial barriers.
While there is an upfront cost, investing in police mental health can reduce long-term expenses related to absenteeism, disability claims, and turnover, while also improving public safety and officer performance.
Officers with better mental health are more likely to make sound decisions, de-escalate situations, and build trust with the community, leading to safer and more positive interactions between law enforcement and the public.