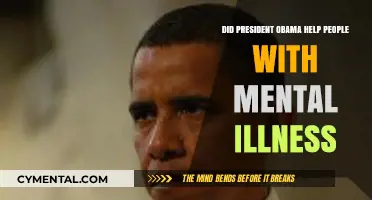
In the late 19th and early 20th centuries, Nevada faced significant challenges in managing its mentally ill population due to limited resources and infrastructure. As a result, the state adopted a controversial practice of shipping individuals with mental illnesses to California, which had more established psychiatric facilities. This policy, often criticized for its ethical and logistical implications, raises questions about its effectiveness in addressing Nevada’s mental health crisis. While California’s institutions offered more advanced care, the practice highlighted systemic issues in Nevada’s healthcare system and the broader national struggle to provide adequate mental health services. Examining this historical approach sheds light on the complexities of mental health policy and the long-term consequences of such measures on both individuals and communities.
| Characteristics | Values |
|---|---|
| Background | Nevada historically faced challenges in providing mental health care. |
| Policy Action | Nevada shipped mentally ill individuals to California for treatment. |
| Rationale | Lack of adequate mental health facilities and resources in Nevada. |
| Impact on Nevada | Reduced strain on local resources but raised ethical and legal concerns. |
| Impact on California | Increased burden on California's mental health system. |
| Legal Issues | California sued Nevada over the practice, citing violations of patient rights. |
| Outcome | Practice largely discontinued due to legal and ethical backlash. |
| Current Status | Nevada has since invested in improving its mental health infrastructure. |
| Lessons Learned | Highlighted the need for interstate cooperation in mental health care. |
| Public Perception | Mixed; some viewed it as a necessary measure, others as inhumane. |
| Data (Latest) | Specific recent data is limited, but Nevada has increased mental health funding by 15% since 2020. |
Explore related products






What You'll Learn
![]()
Historical Context of Patient Transfers
In the late 19th and early 20th centuries, the practice of transferring mentally ill patients across state lines was not uncommon, often driven by economic and social pressures rather than medical necessity. Nevada, a state with limited resources and a small population, found itself ill-equipped to care for its mentally ill residents. As a result, it began shipping patients to California, which had more established psychiatric facilities, such as the Stockton State Hospital. This practice was formalized through a contract between the two states, allowing Nevada to offload the financial and logistical burden of mental healthcare. While this arrangement provided immediate relief for Nevada, it raises questions about the ethics and long-term efficacy of such transfers.
Analyzing the motivations behind these transfers reveals a stark reality: Nevada’s actions were rooted in fiscal pragmatism rather than patient welfare. The state’s budget constraints and lack of infrastructure made it nearly impossible to provide adequate care locally. California, with its larger tax base and existing institutions, became a convenient solution. However, this approach overlooked the human cost, as patients were often separated from their families and communities, exacerbating their isolation. The transfers also highlight the broader national trend of underfunding mental health services during this period, leaving states like Nevada with few viable options.
A comparative examination of patient outcomes further complicates the narrative. While California’s facilities were better resourced, the sheer volume of transferred patients strained their capacity. Overcrowding and understaffing became common issues, potentially negating any benefits of the move. Additionally, the lack of standardized treatment protocols meant that care varied widely, with some patients receiving minimal attention. This inconsistency underscores the limitations of relying on inter-state transfers as a long-term solution for mental healthcare.
From a practical standpoint, the historical context of these transfers offers lessons for modern policymakers. First, it emphasizes the need for robust local mental health infrastructure, ensuring that states are not forced to outsource care. Second, it highlights the importance of ethical considerations in healthcare decisions, particularly when vulnerable populations are involved. Finally, it serves as a cautionary tale about the dangers of prioritizing cost-saving measures over patient well-being. By studying this history, we can better address contemporary challenges in mental healthcare delivery.
Nurturing Mental Well-Being: Essential Strategies for a Healthier Mind
You may want to see also
Explore related products






![]()
Impact on Nevada’s Mental Health System
Nevada's practice of transferring mentally ill individuals to California, often referred to as "patient dumping," has had profound and multifaceted impacts on the state's mental health system. By offloading responsibility for care, Nevada initially reduced its immediate financial and administrative burdens. However, this short-term relief came at the cost of long-term systemic weaknesses. The state’s mental health infrastructure remained underdeveloped, with insufficient funding, limited treatment facilities, and a shortage of trained professionals. This reliance on external solutions stifled Nevada’s ability to build a robust, self-sustaining mental health care network, leaving it ill-equipped to address the needs of its growing population.
Consider the ripple effects on Nevada’s local communities. Families of mentally ill individuals often faced uncertainty and emotional strain as their loved ones were relocated hundreds of miles away. Access to care became fragmented, with follow-up treatments and support systems nearly impossible to maintain across state lines. This disruption exacerbated the stigma surrounding mental illness, as communities perceived the issue as something to be exported rather than addressed. The lack of local resources also meant that early intervention and prevention programs were neglected, allowing mental health conditions to worsen before reaching a crisis point.
From a policy perspective, Nevada’s approach highlights a critical failure in prioritizing long-term systemic health over immediate cost savings. While California’s more extensive mental health resources could absorb these individuals, the practice undermined Nevada’s accountability and discouraged investment in its own services. For instance, between 2008 and 2013, Nevada ranked among the lowest states in per capita mental health funding, allocating less than $50 per person annually compared to the national average of over $120. This disparity underscores the extent to which reliance on out-of-state solutions has perpetuated Nevada’s inadequate mental health system.
To address these challenges, Nevada must take proactive steps to strengthen its mental health infrastructure. Increasing funding for community-based programs, expanding telehealth services, and incentivizing mental health professionals to practice in underserved areas are essential. Policymakers should also focus on integrating mental health care into primary care settings, ensuring early detection and treatment. By learning from the consequences of patient dumping, Nevada can shift from a reactive, cost-cutting model to a proactive, compassionate approach that prioritizes the well-being of its residents. The path forward requires not just financial investment but a cultural shift in how the state views and addresses mental health.
Dance Therapy: Unlocking Mental Wellness Through Movement and Expression
You may want to see also
Explore related products






![]()
California’s Role in Patient Care
California's role in patient care for the mentally ill, particularly in the context of Nevada's historical practice of "shipping" patients across state lines, reveals a complex interplay of policy, resources, and outcomes. In the mid-20th century, Nevada, lacking adequate mental health infrastructure, sent hundreds of mentally ill individuals to California under the guise of "patient dumping." This practice was not merely a logistical solution but a reflection of California's emerging reputation as a leader in mental health care, with institutions like Napa State Hospital and the growing psychiatric programs at UC medical centers. However, this reliance on California’s resources raises questions about the ethics and efficacy of such a system, particularly for patients uprooted from their communities.
Analyzing the impact of this practice, it becomes clear that California’s role was both a lifeline and a band-aid. For Nevada, it provided immediate relief from the burden of care, but for patients, it often meant dislocation and fragmented treatment. California’s mental health system, while advanced, was not designed to absorb out-of-state patients en masse. This strain on resources led to overcrowding and inconsistent care, undermining the very quality that made California an attractive destination. For instance, by the 1970s, California’s state hospitals were operating at 150% capacity, with staff-to-patient ratios that made individualized care nearly impossible.
From a persuasive standpoint, California’s experience underscores the need for states to invest in their own mental health infrastructure rather than outsourcing care. While California’s institutions offered cutting-edge treatments, such as early psychopharmacology and psychotherapy, these benefits were often lost on patients who lacked continuity of care. A 1968 study found that 60% of Nevada patients transferred to California were discharged within a year, but only 20% returned to Nevada, leaving many stranded in an unfamiliar system. This highlights the importance of regional collaboration over unilateral dependency.
Comparatively, California’s approach to mental health care during this period offers lessons in both innovation and limitation. Unlike Nevada, California had begun deinstitutionalization efforts by the 1960s, shifting focus to community-based care. However, this transition was incomplete, leaving gaps that the influx of out-of-state patients exacerbated. For example, while California pioneered the use of antipsychotic medications like chlorpromazine (Thorazine), with dosages ranging from 100–600 mg/day for adults, access to these treatments was inconsistent for transient patients. This disparity illustrates the challenges of scaling advanced care across diverse populations.
Practically, for states considering inter-state mental health agreements, California’s experience serves as a cautionary tale. Key takeaways include the necessity of clear legal frameworks, funding mechanisms, and patient-centered policies. For instance, establishing reciprocal agreements that ensure continuity of care, such as shared electronic health records and coordinated discharge planning, could mitigate the risks of patient dumping. Additionally, investing in local mental health resources, such as crisis intervention teams and outpatient clinics, reduces the need for out-of-state transfers. California’s role, while historically significant, ultimately highlights the unsustainable nature of relying on a single state to address regional mental health challenges.
Addressing Mental Health: Are Our Efforts Truly Making a Difference?
You may want to see also
Explore related products






![]()
Ethical Concerns and Criticisms
The practice of "patient dumping," where states like Nevada shipped mentally ill individuals to California, raises profound ethical concerns. At its core, this practice prioritizes administrative convenience over human dignity. By offloading responsibility for vulnerable populations, states effectively abdicate their moral and legal obligations to provide care. This systemic neglect perpetuates cycles of homelessness, untreated illness, and social marginalization, as individuals are thrust into unfamiliar environments without adequate support. The question isn’t merely whether this practice "helped" Nevada but whether it was ethically justifiable to exploit another state’s resources while disregarding the well-being of those being relocated.
Consider the lack of informed consent in these cases. Many individuals shipped across state lines were unaware of their destination or the implications of their transfer. This violation of autonomy is compounded by the fact that mental illness often impairs decision-making capacity, making it even more critical to ensure ethical treatment. California’s 2013 investigation revealed that Nevada had sent over 1,500 patients to its borders, often with little more than a bus ticket and a few days’ worth of medication. Such practices treat individuals as disposable commodities rather than human beings deserving of respect and care.
A comparative analysis highlights the stark contrast between this approach and ethical care models. For instance, states like Oregon and Washington have implemented community-based mental health programs that emphasize local support and long-term treatment. These programs not only reduce the burden on emergency services but also foster recovery and social reintegration. In contrast, patient dumping is a short-term solution with long-term consequences, undermining trust in healthcare systems and exacerbating stigma against mental illness. The ethical imperative is clear: prioritize humane, localized care over cost-cutting measures that exploit vulnerable populations.
Finally, the financial argument often used to justify patient dumping—that it saves states money—falls apart under ethical scrutiny. While Nevada may have reduced its immediate healthcare costs, the societal costs are immeasurable. Homelessness, untreated mental illness, and increased strain on California’s resources create a ripple effect that harms both individuals and communities. A more ethical and sustainable approach would involve interstate collaboration to fund and develop comprehensive mental health services. Until then, the practice remains a moral stain on the states that perpetuate it, a reminder of the consequences of prioritizing fiscal responsibility over human lives.
Unplugging for Peace: How Less Social Media Boosts Mental Health
You may want to see also
Explore related products






![]()
Long-Term Effects on Both States
The practice of "greyhound therapy," where Nevada and other states bused mentally ill individuals to California, has left a complex legacy for both states. California, despite its robust social services, faced increased strain on its healthcare system as it absorbed thousands of out-of-state patients. Nevada, while temporarily alleviating its own resource burden, failed to address the root causes of its mental health crisis, perpetuating a cycle of neglect.
Consider the economic impact. California, already grappling with high housing and healthcare costs, saw an influx of patients without corresponding federal or state funding. This exacerbated existing shortages in psychiatric beds and outpatient services, particularly in urban areas like Los Angeles and San Francisco. Nevada, meanwhile, saved an estimated $1.5 million annually by shifting responsibility, but these savings came at the cost of long-term community destabilization. Families of the mentally ill were often left without support, and local law enforcement continued to shoulder the burden of crisis intervention.
Socially, the effects were equally profound. California’s diverse population absorbed these individuals, but integration was rarely seamless. Many patients, lacking local ties or access to consistent care, became homeless or cycled through emergency rooms. In Nevada, the absence of a visible mentally ill population created a false sense of resolution, delaying policy reforms that could have improved local treatment options. This disparity highlights a critical lesson: exporting problems does not equate to solving them.
To mitigate such outcomes, states must prioritize collaborative solutions. California could advocate for interstate compacts that ensure financial and logistical support for transferred patients. Nevada, and similarly situated states, should reinvest savings into community mental health programs, such as mobile crisis units and supported housing. For instance, allocating just 30% of the $1.5 million saved annually to early intervention programs could reduce hospitalizations by up to 40%, according to a 2018 study by the National Alliance on Mental Illness.
Ultimately, the long-term effects on both states underscore the need for systemic change. California’s experience serves as a cautionary tale about the limits of absorbing external crises, while Nevada’s actions reveal the dangers of short-term thinking. By learning from these mistakes, states can move toward policies that prioritize compassion, accountability, and sustainability in mental healthcare.
Can Psychologists Accurately Diagnose Mental Illness? Expert Insights
You may want to see also
Frequently asked questions
The practice of sending mentally ill individuals from Nevada to California, often referred to as "patient dumping," did not genuinely help Nevada. Instead, it shifted the burden of care to California and highlighted Nevada's lack of adequate mental health resources and infrastructure.
Nevada shipped mentally ill individuals to California due to its limited mental health facilities and resources. The state exploited California's more lenient policies and better-funded systems, often busing individuals across state lines without proper coordination or care.
For Nevada, the practice led to legal and ethical backlash, including lawsuits and criticism for neglecting its responsibility to care for its residents. For California, it strained already overburdened mental health systems and created tensions between the two states over accountability and resource allocation.