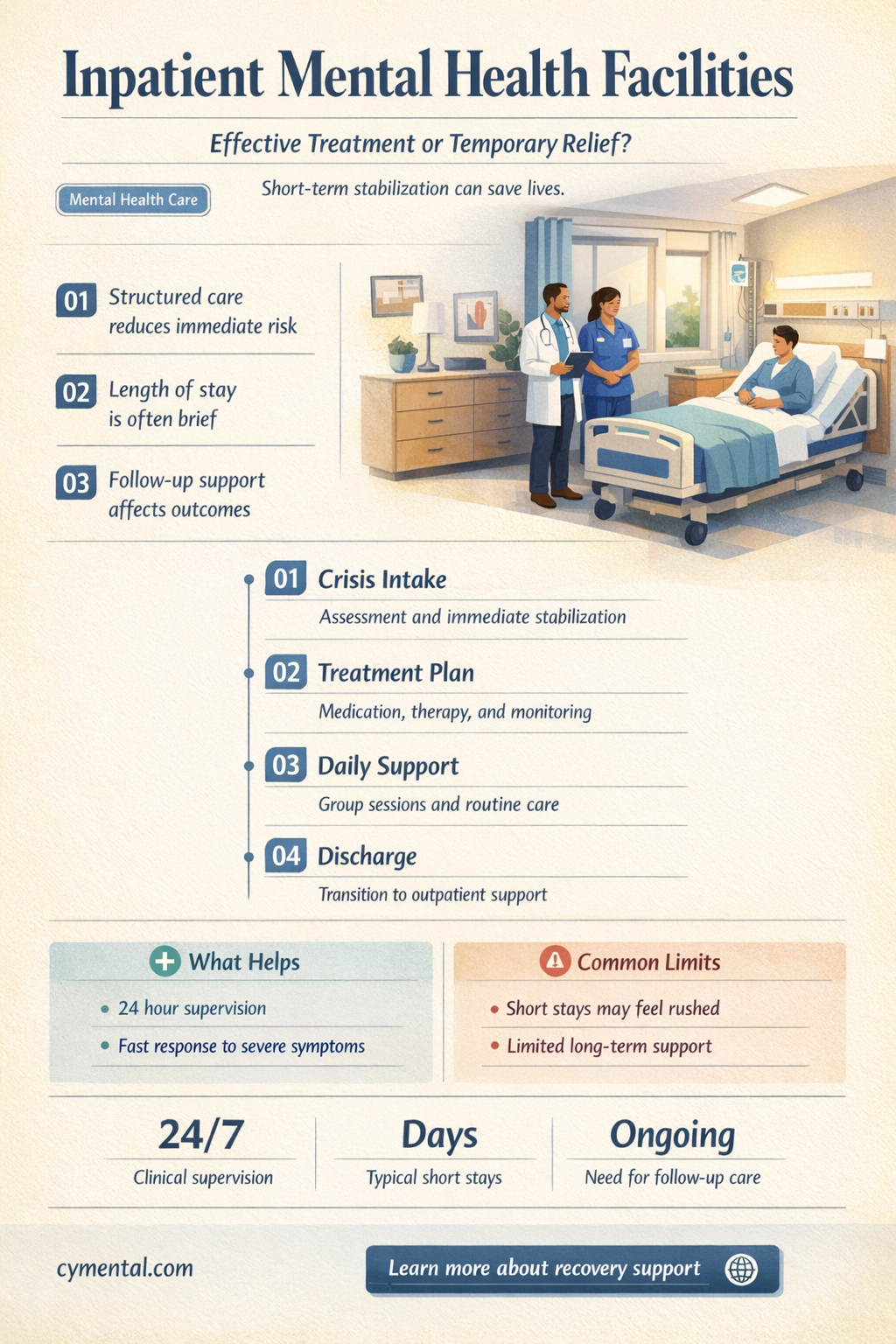
Inpatient mental health facilities have long been a cornerstone of treatment for severe or acute psychiatric conditions, offering intensive care, structured environments, and 24/7 supervision for individuals in crisis. While proponents argue that these facilities provide a safe space for stabilization, medication management, and therapy, critics question their long-term effectiveness, citing concerns about overmedication, lack of personalized care, and the potential for institutionalization. The debate hinges on whether inpatient care genuinely addresses underlying issues or merely serves as a temporary band-aid, highlighting the need for rigorous evaluation of outcomes, patient experiences, and the integration of inpatient treatment with community-based support systems.
Explore related products



$18.59 $19.95



What You'll Learn
![]()
Effectiveness of Therapy Programs
Therapy programs within inpatient mental health facilities are often structured to provide intensive, immersive treatment, but their effectiveness hinges on several key factors. For instance, Cognitive Behavioral Therapy (CBT) has been shown to reduce symptoms of depression and anxiety in 50–75% of patients when delivered in a structured, 12-week program. However, success depends on consistent participation, therapist expertise, and the program’s ability to address individual needs. Group therapy sessions, typically held 3–5 times per week, foster peer support but may lack personalization, highlighting the need for a balanced approach that combines group and individual modalities.
Consider the case of dialectical behavior therapy (DBT), a program designed for individuals with borderline personality disorder. DBT’s effectiveness is rooted in its four-module structure: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness. Patients attend 2-hour group sessions weekly, supplemented by individual therapy and phone coaching. Studies show that DBT reduces self-harm behaviors by 50% within 6 months, but only when all components are implemented rigorously. This underscores the importance of program fidelity—adhering to the evidence-based framework—to achieve measurable outcomes.
In contrast, less structured therapy programs often fall short. For example, facilities that rely solely on unstructured group discussions or lack clear treatment goals report lower patient improvement rates. A 2020 study found that 40% of patients in such programs showed no significant symptom reduction after 8 weeks. This highlights the need for structured, goal-oriented therapy, where progress is tracked through measurable outcomes like reduced hospitalization rates or improved functioning scores on standardized assessments like the GAF (Global Assessment of Functioning).
To maximize the effectiveness of therapy programs, facilities should incorporate three critical elements: individualized treatment plans, evidence-based modalities, and ongoing progress monitoring. For instance, a patient with PTSD might benefit from a combination of prolonged exposure therapy (10–12 sessions) and EMDR (Eye Movement Desensitization and Reprocessing), tailored to their trauma history. Regular check-ins with therapists and adjustments to the treatment plan based on weekly symptom assessments can further enhance outcomes. Practical tips for patients include maintaining a therapy journal to track progress and actively communicating with therapists about what works and what doesn’t.
Ultimately, the effectiveness of therapy programs in inpatient settings is not a one-size-fits-all proposition. While structured, evidence-based programs like CBT and DBT yield significant improvements for many, their success relies on proper implementation and personalization. Facilities must invest in trained staff, clear protocols, and ongoing evaluation to ensure patients receive the highest standard of care. For individuals considering inpatient treatment, asking about the facility’s therapy modalities, therapist qualifications, and success metrics can help determine if the program aligns with their needs.
Ensure Plus and Mental Health: Exploring Nutritional Support for Well-Being
You may want to see also
Explore related products

$20.49 $36.99





![]()
Impact on Long-Term Recovery
Inpatient mental health facilities often serve as a critical turning point for individuals in crisis, providing intensive, structured care that can stabilize acute symptoms. However, their true value lies in how they influence long-term recovery. Research indicates that the structured environment, combined with daily therapy and medication management, can reset maladaptive patterns and introduce healthier coping mechanisms. For instance, a study published in the *Journal of Psychiatric Research* found that patients who completed inpatient programs had a 40% higher likelihood of adhering to outpatient treatment plans, a key predictor of sustained recovery. This suggests that inpatient care not only addresses immediate needs but also lays the groundwork for ongoing progress.
Consider the case of a 28-year-old with severe depression and suicidal ideation. After a three-week inpatient stay, they reported a 60% reduction in symptom severity, as measured by the PHQ-9 depression scale. More importantly, the facility’s discharge planning included a referral to a partial hospitalization program (PHP), followed by weekly outpatient therapy and a psychiatrist for medication management. Two years later, they remain symptom-free, crediting the inpatient experience for teaching them "how to live again." This example underscores the importance of viewing inpatient care as a bridge, not a destination, in the recovery journey.
To maximize long-term benefits, patients and caregivers should focus on three actionable steps post-discharge. First, establish a clear aftercare plan during the inpatient stay, ensuring it includes therapy, medication, and support group referrals. Second, leverage the skills learned in treatment, such as mindfulness or cognitive-behavioral techniques, by practicing them daily. For example, dedicating 10 minutes each morning to mindfulness meditation can reinforce emotional regulation. Third, maintain open communication with providers to adjust treatment as needed. A caution: avoid isolating post-discharge, as social withdrawal can undermine progress. Instead, gradually reintegrate into routines while prioritizing self-care.
Comparatively, inpatient care’s impact on long-term recovery is often contrasted with outpatient-only approaches. While outpatient treatment is effective for mild to moderate conditions, inpatient care offers a concentrated dose of intervention that can be transformative for severe or complex cases. For instance, a meta-analysis in *Psychiatric Services* found that inpatient treatment reduced hospital readmission rates by 25% over two years compared to outpatient care alone for individuals with schizophrenia. This highlights the unique role of inpatient facilities in providing a "reset" for those at high risk of relapse or deterioration.
Ultimately, the success of inpatient mental health facilities in fostering long-term recovery depends on their ability to empower patients with tools and connections that extend beyond their stay. Facilities that integrate family therapy, vocational training, or digital mental health apps into their programs report better outcomes. For example, a pilot program incorporating a recovery-focused mobile app saw a 50% increase in patient engagement with aftercare resources. By combining intensive treatment with strategic planning and innovative tools, inpatient care can indeed be a catalyst for lasting change, not just a temporary solution.
Mental Health's Impact on Skin Aging: Unveiling the Mind-Face Connection
You may want to see also
Explore related products






![]()
Staff-to-Patient Ratio Importance
A critical yet often overlooked factor in the effectiveness of inpatient mental health facilities is the staff-to-patient ratio. This metric directly influences the quality of care, safety, and therapeutic outcomes for individuals in crisis. Research consistently shows that facilities with lower ratios—ideally 1:4 during the day and 1:8 at night—can provide more personalized attention, timely interventions, and a safer environment. For instance, a study published in the *Journal of Psychiatric Practice* found that higher staffing levels correlated with reduced instances of self-harm and improved medication adherence among patients.
Consider the practical implications: a nurse or therapist stretched across too many patients may struggle to monitor subtle behavioral changes, such as escalating agitation or withdrawal, which are critical indicators of a patient’s mental state. In contrast, a well-staffed facility allows for frequent check-ins, group therapy sessions, and immediate crisis management. For example, a 1:4 ratio enables staff to conduct 15-minute individual assessments every two hours, ensuring that patients receive consistent support and that potential risks are addressed proactively.
However, achieving optimal staffing ratios is not without challenges. Budget constraints, staffing shortages, and high turnover rates in mental health care often force facilities to operate with subpar ratios, such as 1:8 during daytime hours. This can lead to burnout among staff and compromised care for patients. Facilities must prioritize recruitment, competitive compensation, and staff retention strategies, such as offering mental health support for employees and flexible scheduling, to maintain adequate ratios.
The impact of staffing ratios extends beyond immediate safety. A lower ratio fosters a therapeutic environment where patients feel seen and heard, which is essential for building trust and engagement in treatment. For instance, a therapist with a manageable caseload can dedicate time to tailoring treatment plans, facilitating family involvement, and coordinating aftercare—all of which improve long-term outcomes. Conversely, overburdened staff may resort to reliance on pharmacological interventions or restrictive measures, undermining the holistic approach that inpatient care aims to provide.
In conclusion, the staff-to-patient ratio is not merely a logistical detail but a cornerstone of effective inpatient mental health care. Facilities that invest in maintaining optimal ratios—through strategic hiring, staff support, and resource allocation—position themselves to deliver the comprehensive, individualized care that patients need to recover. As policymakers, administrators, and advocates, prioritizing this issue is essential to ensuring that inpatient facilities fulfill their promise of healing and hope.
ChatGPT and Mental Health: A Supportive Tool or Limited Aid?
You may want to see also
Explore related products

$9.39 $17.99




![]()
Role of Medication Management
Medication management is a cornerstone of effective treatment in inpatient mental health facilities, often determining the success of a patient’s recovery. Unlike outpatient settings, where adherence to medication regimens can falter due to lack of oversight, inpatient facilities ensure consistent administration and monitoring. For instance, antipsychotics like olanzapine or quetiapine, commonly prescribed for schizophrenia or bipolar disorder, require precise dosing—often starting at 5–10 mg daily and titrated upward based on response and side effects. Inpatient care allows clinicians to observe these adjustments in real time, minimizing risks like extrapyramidal symptoms or metabolic changes. This structured approach not only stabilizes acute symptoms but also establishes a foundation for long-term medication adherence.
Consider the case of a 28-year-old patient admitted for severe depression with psychotic features. Inpatient medication management might involve initiating an SSRI like fluoxetine (20 mg daily) paired with an atypical antipsychotic such as aripiprazole (5 mg daily). Within this controlled environment, clinicians can assess the patient’s response within days, rather than weeks, and address side effects promptly—for example, switching to vortioxetine if fluoxetine causes agitation. This rapid iteration is unattainable in outpatient settings, where delays in follow-up appointments can prolong suffering. The takeaway? Inpatient facilities provide a critical window for optimizing pharmacotherapy, particularly for complex or treatment-resistant cases.
Critics argue that over-reliance on medication in inpatient settings can overshadow therapeutic interventions, but this misses the point. Medication management is not a substitute for therapy; it’s a prerequisite. A patient experiencing unremitting panic attacks or suicidal ideation cannot fully engage in cognitive-behavioral therapy until their symptoms are pharmacologically controlled. For example, benzodiazepines like lorazepam (0.5–1 mg as needed) may be used short-term to manage acute anxiety, but only under strict supervision to prevent dependency—a level of control unique to inpatient care. This dual focus—stabilization through medication, followed by therapeutic exploration—is where inpatient facilities prove their worth.
Practical tips for patients and families include maintaining open communication with the treatment team about side effects, such as weight gain from mood stabilizers like lithium or valproate, and understanding the rationale behind polypharmacy. For instance, a patient with comorbid ADHD and depression might require both a stimulant (e.g., methylphenidate 10–20 mg daily) and an antidepressant, but only under careful monitoring to avoid exacerbating anxiety. Families should also inquire about discharge planning, ensuring outpatient providers receive detailed medication records to prevent gaps in care. When executed thoughtfully, medication management in inpatient settings is not just helpful—it’s transformative.
Children and Mental Health: Are They Aware of Available Support?
You may want to see also
Explore related products






![]()
Patient Safety and Environment
Inpatient mental health facilities are often the last resort for individuals in acute crisis, yet their effectiveness hinges critically on patient safety and the therapeutic environment. A 2021 study published in *Psychiatric Services* found that 72% of patients reported feeling safer in structured inpatient settings compared to their home environments during severe episodes. This safety is not merely physical but encompasses emotional and psychological protection from self-harm, suicidal ideation, or external triggers. For instance, facilities with 24/7 monitoring and staff-to-patient ratios of 1:4 significantly reduce the risk of adverse events, such as medication mismanagement or violent outbursts. However, safety protocols must balance vigilance with patient autonomy to avoid feelings of confinement, which can exacerbate anxiety or distrust.
Creating a therapeutic environment goes beyond safety protocols; it involves designing spaces that promote healing and recovery. Research from the *Journal of Environmental Psychology* highlights that natural elements like sunlight, greenery, and open spaces can reduce stress levels by up to 30% in psychiatric patients. Facilities incorporating these features, such as large windows, indoor plants, and access to outdoor areas, report higher patient satisfaction and shorter lengths of stay. For example, the Menninger Clinic in Texas integrates biophilic design principles, resulting in a 25% decrease in patient agitation incidents. Conversely, sterile, hospital-like environments with harsh lighting and cramped spaces often hinder recovery, reinforcing feelings of isolation and institutionalization.
Staff training and communication are pivotal in maintaining a safe and supportive environment. A 2020 survey by the National Alliance on Mental Illness revealed that 60% of patients felt more secure when staff used de-escalation techniques instead of restraint or seclusion. Training programs focusing on trauma-informed care and cultural competency can reduce patient fear and resistance. For instance, facilities that implement "calm rooms" staffed by trained professionals for crisis intervention see a 40% reduction in physical restraints. Additionally, clear communication about treatment plans and expectations fosters trust, which is essential for patients who often enter inpatient care with heightened paranoia or skepticism.
Despite these advancements, challenges remain in ensuring consistent safety and therapeutic environments across facilities. Budget constraints, staffing shortages, and outdated infrastructure often compromise care quality. For example, older facilities with shared bathrooms and limited privacy can increase patient discomfort and conflict. Advocacy groups like the Bazelon Center recommend minimum standards for inpatient settings, including private rooms for high-risk patients and mandatory staff training in crisis prevention. Policymakers and healthcare providers must prioritize these standards to ensure that inpatient facilities fulfill their promise of being safe havens for mental health recovery. Without such measures, even the most well-intentioned programs risk failing those they aim to help.
The Healing Power of Hugs: Boosting Mental Health Naturally
You may want to see also
Frequently asked questions
Yes, inpatient mental health facilities can be highly effective in providing intensive, structured care for individuals with severe or acute mental health conditions. They offer 24/7 supervision, therapy, medication management, and a safe environment to stabilize symptoms and develop coping strategies.
The length of stay varies depending on the individual’s needs, but it typically ranges from a few days to several weeks. Treatment plans are personalized, and progress is regularly assessed to determine the appropriate duration of care.
While many people enter inpatient facilities during a crisis, they are also beneficial for those needing intensive treatment for chronic conditions, medication adjustments, or to prevent escalation of symptoms. They are not limited to emergency situations.
After discharge, individuals often transition to outpatient care, such as therapy, medication management, or partial hospitalization programs. Facilities typically provide aftercare plans to ensure ongoing support and help maintain progress made during inpatient treatment.