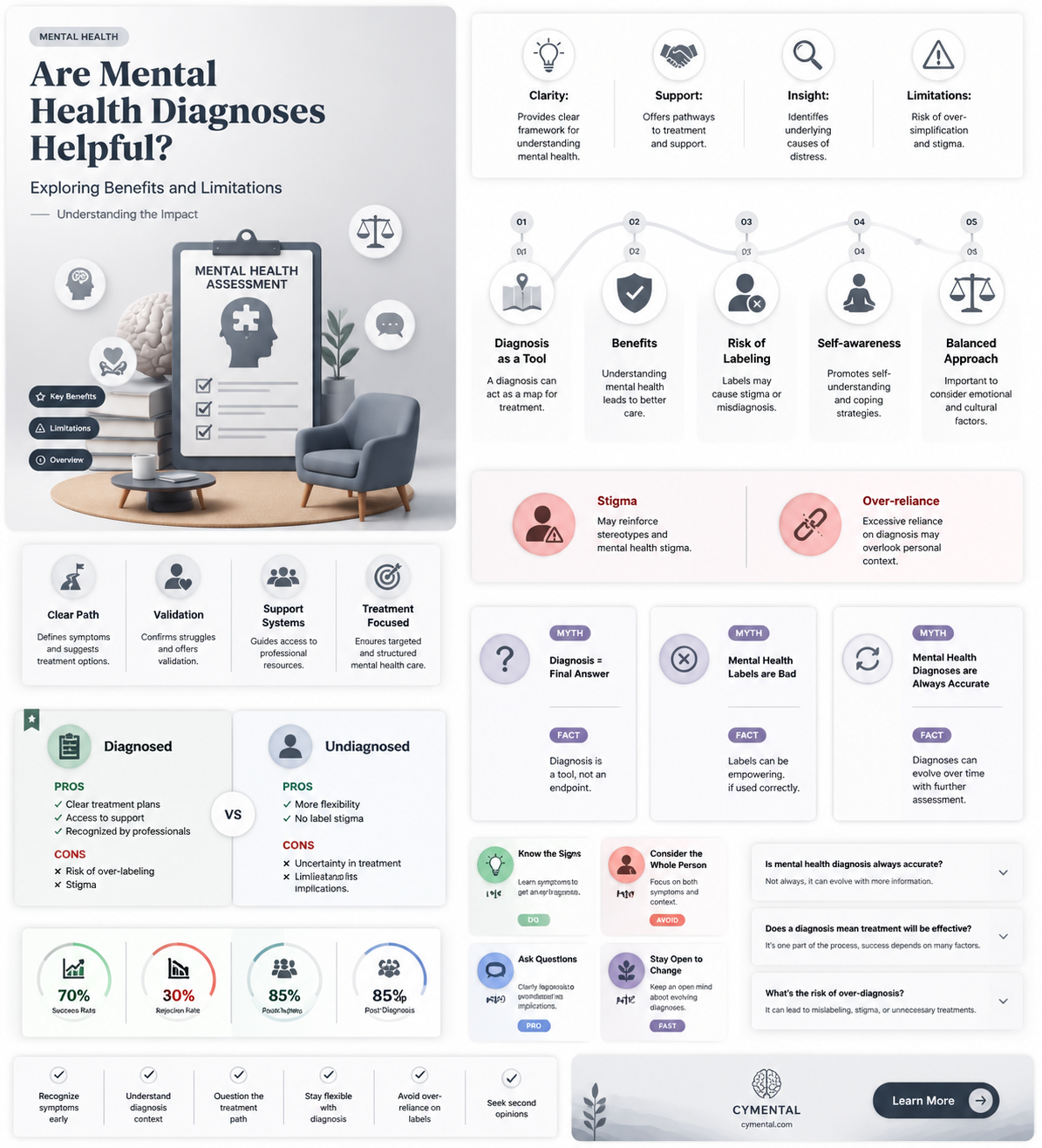
The question of whether mental health diagnoses are helpful is a complex and multifaceted one, sparking debates among professionals, patients, and advocates alike. On one hand, diagnoses can provide a framework for understanding symptoms, guiding treatment, and offering validation to individuals who may feel isolated or misunderstood. They can also facilitate access to resources, insurance coverage, and support systems. However, critics argue that diagnoses may oversimplify the intricate nature of human experience, potentially leading to stigmatization, misdiagnosis, or over-reliance on labels. Additionally, the subjective nature of some diagnostic criteria raises concerns about consistency and cultural biases. Ultimately, the value of a mental health diagnosis depends on how it is used—whether as a tool for empowerment and healing or as a limiting label that reduces an individual’s identity to a set of symptoms.
Explore related products






What You'll Learn
![]()
Accuracy of Diagnoses
Mental health diagnoses are often seen as the first step toward treatment, but their accuracy remains a critical concern. Misdiagnosis can lead to inappropriate interventions, delayed care, or unnecessary stigma. For instance, a study published in the *Journal of Clinical Psychiatry* found that up to 20% of patients initially diagnosed with major depressive disorder were later reclassified with bipolar disorder, a condition requiring fundamentally different treatment approaches. Such discrepancies highlight the complexity of mental health conditions and the limitations of current diagnostic tools.
Consider the diagnostic process itself, which relies heavily on self-reported symptoms and clinical judgment. Unlike physical illnesses, mental health disorders lack definitive biomarkers, making diagnoses subjective and prone to error. For example, ADHD and anxiety disorders share overlapping symptoms like restlessness and difficulty concentrating, often leading to confusion during assessment. Clinicians must meticulously differentiate between these conditions, sometimes requiring months of observation or additional testing, which can delay effective treatment.
To improve accuracy, some experts advocate for integrating quantitative measures into diagnostics. Tools like standardized questionnaires (e.g., the PHQ-9 for depression) or neuroimaging techniques (e.g., fMRI for identifying brain activity patterns) can provide objective data to complement clinical interviews. However, these methods are not foolproof. Questionnaires rely on patient honesty and self-awareness, while neuroimaging is expensive and not widely accessible. Balancing these tools with clinical expertise remains essential but challenging.
A practical tip for individuals seeking a diagnosis is to maintain a detailed symptom journal. Record daily experiences, triggers, and changes in behavior or mood over several weeks. This documentation can provide clinicians with a clearer picture of your condition, reducing the likelihood of misdiagnosis. Additionally, seeking a second opinion from a different specialist can offer valuable perspective, especially if initial treatment proves ineffective.
Ultimately, the accuracy of mental health diagnoses hinges on a combination of rigorous assessment, patient involvement, and ongoing refinement of diagnostic criteria. While current methods are imperfect, they remain a necessary foundation for personalized care. As research advances, the hope is that diagnoses will become more precise, minimizing harm and maximizing the benefits of treatment. Until then, vigilance and collaboration between patients and providers are key to navigating this complex landscape.
Seeking Support: A Guide to Accessing Mental Health Assistance
You may want to see also
Explore related products



$32.99 $32.99



![]()
Impact on Treatment Plans
A mental health diagnosis can significantly influence the trajectory of treatment, often determining the modalities, medications, and therapeutic approaches used. For instance, a diagnosis of Major Depressive Disorder (MDD) typically leads to a treatment plan that includes selective serotonin reuptake inhibitors (SSRIs) like fluoxetine (20–60 mg/day) or cognitive-behavioral therapy (CBT). Without a clear diagnosis, clinicians might resort to trial-and-error methods, delaying effective relief. This precision in treatment planning underscores the practical utility of diagnoses in streamlining care.
Consider the case of anxiety disorders, where generalized anxiety disorder (GAD) and panic disorder, though overlapping in symptoms, require distinct interventions. GAD often responds to long-term therapies like CBT or medications such as venlafaxine (75–225 mg/day), whereas panic disorder may benefit from short-term benzodiazepines like alprazolam (0.25–2 mg/day) alongside exposure therapy. A misdiagnosis could lead to inappropriate prescriptions, such as using benzodiazepines for GAD, which carry risks of dependence. Here, the diagnosis acts as a safeguard, ensuring treatments align with the disorder’s unique demands.
However, diagnoses are not without limitations. For children and adolescents, where developmental factors complicate symptom presentation, a rigid diagnosis might lead to over-reliance on medication. For example, ADHD diagnoses in children aged 6–12 often result in stimulant prescriptions like methylphenidate (10–60 mg/day), but without concurrent behavioral interventions, long-term outcomes may suffer. Clinicians must balance diagnostic clarity with flexibility, integrating age-specific considerations into treatment plans.
In practice, a diagnosis serves as a starting point, not an endpoint. For instance, a diagnosis of bipolar disorder necessitates mood stabilizers like lithium (600–1200 mg/day) but requires careful monitoring for side effects such as thyroid dysfunction. Similarly, PTSD treatment plans often include trauma-focused therapies like prolonged exposure (PE) or eye movement desensitization and reprocessing (EMDR), tailored to the individual’s trauma history. The diagnosis provides a framework, but personalization remains key to efficacy.
Ultimately, the impact of a diagnosis on treatment plans is twofold: it provides direction while demanding adaptability. Clinicians must use diagnoses as tools to guide evidence-based interventions but remain vigilant to individual nuances. For patients, understanding their diagnosis empowers them to engage in treatment decisions, fostering collaboration. In this way, diagnoses are not merely labels but catalysts for informed, effective care.
Seeking Mental Health Support: A Guide to Finding the Right Help
You may want to see also
Explore related products



$22.2 $46



![]()
Stigma and Labeling Effects
Mental health diagnoses can inadvertently become self-fulfilling prophecies, shaping how individuals perceive themselves and are perceived by others. When a person is labeled with a condition like "depression" or "anxiety disorder," this label often becomes a central part of their identity, influencing their behaviors and expectations. For instance, a teenager diagnosed with social anxiety might avoid social situations more rigidly, fearing confirmation of the diagnosis, thereby reinforcing the very symptoms they aim to manage. This phenomenon, known as the "labeling effect," highlights how diagnoses, while intended to guide treatment, can sometimes limit potential and foster dependency on the diagnosis itself.
Consider the workplace, where stigma surrounding mental health diagnoses can lead to tangible discrimination. An employee diagnosed with bipolar disorder might be passed over for promotions or leadership roles, not due to performance but because of assumptions about unpredictability or unreliability. Such stigma is often rooted in misinformation and fear, perpetuated by media portrayals and cultural stereotypes. For example, a study by the American Psychiatric Association found that 60% of employees fear disclosing mental health issues due to potential negative career consequences. This reluctance to disclose can delay treatment and exacerbate symptoms, creating a cycle of silence and suffering.
To mitigate labeling effects, clinicians and individuals must adopt a nuanced approach to diagnosis. Instead of viewing diagnoses as rigid categories, they should be seen as tools for understanding and addressing specific symptoms. For instance, a diagnosis of "generalized anxiety disorder" could be reframed as "experiencing heightened worry and physical tension in response to stressors." This shifts the focus from the label to the experience, reducing the risk of internalized stigma. Additionally, incorporating strengths-based language—such as highlighting resilience or coping mechanisms—can empower individuals to see beyond their diagnosis.
Practical steps can also be taken to combat stigma at systemic levels. Employers can implement policies that promote mental health awareness and provide resources like Employee Assistance Programs (EAPs) or flexible work arrangements. Schools can integrate mental health education into curricula, fostering empathy and reducing bullying. On a personal level, individuals can challenge stigmatizing language in conversations, replacing phrases like "she’s schizophrenic" with "she lives with schizophrenia." These small but intentional changes can reshape societal attitudes and reduce the isolating effects of labeling.
Ultimately, while mental health diagnoses serve as crucial starting points for treatment, their impact depends on how they are communicated and perceived. By acknowledging the risks of stigma and labeling, we can transform diagnoses from limiting labels into catalysts for understanding, support, and growth. This requires collective effort—from healthcare providers to policymakers to everyday individuals—to create environments where diagnoses are tools for empowerment, not chains of limitation.
Supporting Veterans: Strategies to Address Mental Health Challenges Effectively
You may want to see also
Explore related products






![]()
Patient Empowerment vs. Dependency
Mental health diagnoses can serve as double-edged swords, offering clarity and direction while risking the creation of limiting labels. On one hand, a diagnosis provides a framework for understanding symptoms, accessing tailored treatments, and validating experiences. For instance, a diagnosis of generalized anxiety disorder can guide a therapist to recommend cognitive-behavioral therapy (CBT) paired with a low-dose SSRI (e.g., 10–20 mg of escitalopram daily), a combination proven effective in 60–70% of cases. On the other hand, labels like "bipolar" or "schizophrenia" can stigmatize, reducing individuals to their conditions rather than acknowledging their multifaceted identities. This tension underscores the debate between patient empowerment and dependency.
Empowerment thrives when diagnoses are used as tools, not chains. A 35-year-old diagnosed with major depressive disorder might leverage this knowledge to advocate for workplace accommodations, such as flexible hours during therapy sessions, or to educate themselves on self-management strategies like mindfulness and sleep hygiene. Here, the diagnosis becomes a starting point for proactive engagement with one’s health. However, empowerment falters when patients are passive recipients of care, relying solely on providers to dictate their treatment paths. For example, a teenager diagnosed with ADHD may internalize the label as an excuse for disorganization rather than using it to explore organizational tools or stimulant medications (e.g., 10–30 mg of methylphenidate daily) that could enhance focus.
Dependency emerges when diagnoses overshadow individual agency, fostering a mindset of permanence rather than possibility. A 50-year-old diagnosed with PTSD might feel trapped by the label, believing their trauma defines their future instead of viewing it as one chapter in their story. This dependency is often reinforced by systemic factors, such as insurance requirements that tie treatment to specific diagnoses, limiting flexibility in care. For instance, a patient seeking therapy for stress may be pressured to accept a diagnosis of adjustment disorder to qualify for coverage, even if the label feels reductive.
To navigate this balance, patients and providers must collaborate to reframe diagnoses as dynamic guides, not static identities. Practical steps include: (1) encouraging patients to ask questions like, "What does this diagnosis mean for my daily life?" rather than "Who am I now?"; (2) integrating holistic approaches, such as peer support groups or art therapy, alongside traditional treatments; and (3) regularly reassessing diagnoses to reflect evolving symptoms and insights. For example, a young adult initially diagnosed with social anxiety disorder might later discover that their symptoms stem from undiagnosed autism, shifting their treatment focus from exposure therapy to sensory regulation techniques.
Ultimately, the value of a mental health diagnosis lies in its ability to empower, not define. By treating diagnoses as starting points for exploration and growth, patients can avoid the pitfalls of dependency, reclaiming their narratives and charting paths toward resilience. This approach requires intentionality from both individuals and systems, but the payoff—a more nuanced, compassionate understanding of mental health—is worth the effort.
Boost Focus and Calm: Strategies for Achieving Mental Clarity
You may want to see also
Explore related products






![]()
Cultural and Social Influences
Cultural and social norms shape how mental health diagnoses are perceived and utilized, often determining their helpfulness in diverse communities. In collectivist cultures, for example, mental health issues may be viewed as family or community responsibilities rather than individual ailments. A diagnosis like depression might prompt communal support systems to activate, offering practical assistance and emotional reassurance. Conversely, in individualistic societies, the focus tends to be on personal accountability and self-improvement, where a diagnosis can serve as a roadmap for targeted therapy or medication. Understanding these cultural frameworks is essential for clinicians and patients alike, as it influences not only acceptance but also adherence to treatment plans.
Consider the role of language and stigma in social settings. In some communities, terms like "anxiety" or "bipolar disorder" carry heavy negative connotations, leading individuals to avoid seeking diagnoses altogether. For instance, in certain African cultures, mental health conditions are sometimes attributed to spiritual causes, making Western diagnostic labels seem irrelevant or even harmful. Here, a diagnosis might only be helpful if it bridges cultural understanding—perhaps by integrating traditional healing practices with modern psychiatric care. Practitioners must navigate these linguistic and conceptual barriers to ensure diagnoses are not just clinically accurate but culturally sensitive.
Social media has emerged as a double-edged sword in this context. On one hand, platforms like Instagram and TikTok have normalized discussions around mental health, encouraging younger demographics (ages 18–34) to seek diagnoses for conditions like ADHD or PTSD. On the other hand, the oversimplification of complex disorders through viral trends can lead to self-misdiagnosis, trivializing the diagnostic process. For example, the hashtag #ADHD has billions of views, yet many users mistake everyday forgetfulness for a clinical disorder. Clinicians now face the challenge of distinguishing between genuine symptoms and social media-induced hypochesis, underscoring the need for rigorous assessment tools that account for social influences.
Finally, socioeconomic factors cannot be overlooked. Access to mental health services is often gated by income, education, and geographic location, making diagnoses less helpful for marginalized groups. In low-income communities, a diagnosis might highlight a problem without offering actionable solutions due to limited resources. For instance, a child diagnosed with autism in a rural area may face long wait times for specialized therapy, rendering the diagnosis more stressful than beneficial. Policymakers and healthcare providers must address these disparities by expanding affordable care options and training culturally competent practitioners to ensure diagnoses translate into meaningful support across all social strata.
In navigating these cultural and social influences, the helpfulness of a mental health diagnosis hinges on its ability to resonate within the individual’s unique context. Clinicians must adopt a nuanced approach, blending clinical expertise with cultural humility, while individuals should advocate for diagnoses that align with their lived experiences. By doing so, diagnoses can transcend mere labels, becoming tools for empowerment rather than alienation.
Finding Support: Where to Go for Help in Difficult Times
You may want to see also
Frequently asked questions
Yes, mental health diagnoses can provide a framework to understand symptoms, identify patterns, and guide appropriate treatment options.
While diagnoses can sometimes lead to stigma or oversimplification, they are tools meant to assist in treatment, not define a person’s identity.
No, diagnoses are starting points; effective treatment depends on individualized care, therapy, and sometimes medication tailored to the person’s needs.
Absolutely. Many people experience mental health challenges without meeting criteria for a specific diagnosis, and support can still be beneficial.