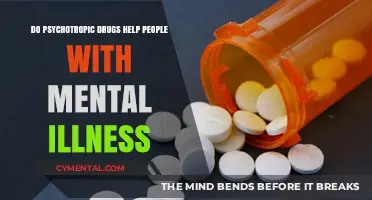
The relationship between sexual fetishes and mental illness is a complex and often misunderstood topic. While some fetishes may be considered atypical or unconventional, they do not inherently indicate mental illness. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) classifies certain fetishes as paraphilic disorders only when they cause significant distress or impairment in an individual's life, involve non-consenting partners, or are associated with harmful behaviors. However, many people with fetishes lead healthy, functional lives, and their interests do not necessarily reflect underlying psychological issues. Distinguishing between a harmless fetish and a potential mental health concern requires careful consideration of context, consent, and the individual's overall well-being, challenging the simplistic notion that fetishes alone can determine mental illness.
| Characteristics | Values |
|---|---|
| Definition of Fetish | A sexual fetish is an intense sexual interest in an object, body part, or situation that is not typically considered sexually arousing. |
| Prevalence | Fetishes are relatively common, with studies suggesting 30-40% of individuals report having a fetish. |
| DSM-5 Classification | Only classified as a disorder (Fetishistic Disorder) if it causes significant distress or impairment in functioning, and if the arousal depends on the presence of the fetish object/situation. |
| Relationship to Mental Illness | Most people with fetishes do not have a mental illness. Fetishes alone are not diagnostic criteria for any mental disorder. |
| Potential Associations | Some research suggests potential links between certain fetishes and specific mental health conditions (e.g., OCD, BDSM and borderline personality traits), but these are correlations, not causations. |
| Stigma and Misconceptions | Fetishes are often stigmatized and misunderstood, leading to shame and reluctance to seek help if needed. |
| Importance of Context | The context and impact of a fetish on an individual's life are crucial in determining if professional help is warranted. |
| Healthy Expression | Fetishes can be expressed in consensual, safe, and healthy ways within relationships. |
| Seeking Help | If a fetish causes distress, interferes with daily life, or involves non-consensual acts, seeking professional help from a sex-positive therapist is recommended. |
Explore related products






What You'll Learn
- Fetish vs. Paraphilia: Distinguishing healthy fetishes from clinically significant paraphilic disorders
- DSM-5 Criteria: How diagnostic manuals classify fetishes related to mental health
- Impact on Functioning: Assessing if fetishes impair daily life or relationships
- Co-occurring Disorders: Links between fetishes and conditions like OCD or PTSD
- Cultural vs. Clinical: Differentiating culturally influenced fetishes from pathological behaviors
![]()
Fetish vs. Paraphilia: Distinguishing healthy fetishes from clinically significant paraphilic disorders
Sexual fetishes, by definition, involve an intense sexual interest in an object, body part, or scenario that may seem unconventional. But when does a fetish cross the line from a quirky preference to a clinical concern? The distinction lies in the impact it has on an individual's life and well-being, marking the difference between a fetish and a paraphilic disorder.
Understanding the Spectrum:
Fetishes are diverse and highly individualized, ranging from a fascination with feet to more complex scenarios like role-playing. These interests become clinically significant when they meet the criteria for paraphilic disorders, as outlined in diagnostic manuals such as the DSM-5. Paraphilia is characterized by intense sexual arousal to atypical objects, situations, or individuals, often causing distress or impairment in social, occupational, or other important areas of functioning. For instance, a person with a foot fetish may enjoy foot-related activities without any negative consequences, but if their obsession leads to stalking or harassing strangers for their feet, it could indicate a paraphilic disorder.
Distinguishing Factors:
The key differentiator is the presence of harm or distress. Healthy fetishes are consensual, private, or shared within a mutually respectful context, enhancing sexual pleasure without causing harm. They are often integrated into a person's sexual repertoire without interfering with their daily life. In contrast, paraphilic disorders can lead to risky behaviors, legal issues, or significant personal distress. For example, a fetish for rubber clothing is harmless until it evolves into a compulsive need to wear it in inappropriate settings, potentially endangering one's job or personal relationships.
Clinical Assessment and Treatment:
Mental health professionals assess paraphilic disorders through comprehensive evaluations, considering the intensity, duration, and impact of the behavior. Treatment is not about eliminating the fetish but managing its expression. Cognitive-behavioral therapy (CBT) is often employed to help individuals understand and control their impulses, especially in cases where the behavior is illegal or harmful. For instance, a treatment plan might involve teaching a person with a public exhibitionism disorder techniques to manage their urges and explore safer outlets for their fetish.
Navigating the Gray Areas:
The line between a fetish and paraphilia can be blurry. Cultural and societal norms play a role in defining what is considered 'atypical' sexual behavior. What might be a fetish in one culture could be a common practice in another. Therefore, clinicians must exercise cultural sensitivity and focus on the individual's experience of distress and impairment rather than judging the fetish itself. It's crucial to approach these topics with an open mind, ensuring that personal biases do not influence the assessment and treatment process.
In summary, while fetishes are a normal part of human sexual diversity, they warrant clinical attention when they cause significant distress or harm. Understanding this distinction is essential for both individuals exploring their sexuality and professionals providing guidance and support. By recognizing the difference between a healthy fetish and a paraphilic disorder, we can promote sexual well-being and ensure that those in need receive appropriate care.
Stuffed Animals: Surprising Mental Health Benefits and Comfort They Offer
You may want to see also
Explore related products






![]()
DSM-5 Criteria: How diagnostic manuals classify fetishes related to mental health
The DSM-5, the diagnostic bible of psychiatry, treads carefully when classifying sexual fetishes. Unlike earlier editions, it avoids pathologizing consensual, non-harmful paraphilias. Instead, it introduces a nuanced framework centered on "Paraphilic Disorders," defined by three critical criteria: distress, functional impairment, and non-consent. This shift reflects a growing understanding that atypical sexual interests alone do not constitute mental illness.
A fetish, in DSM-5 terms, becomes a disorder only when it causes significant personal suffering, interferes with daily life, or involves non-consensual acts. For example, a foot fetishist who enjoys consensual foot-related activities without distress wouldn't meet the criteria. Conversely, someone whose fetish leads to social isolation, job loss, or compulsive behaviors harming others would likely qualify for diagnosis. This distinction is crucial, as it prevents stigmatizing harmless variations in human sexuality while identifying cases requiring intervention.
The DSM-5's approach is instructive for both clinicians and the public. It encourages a move away from moral judgment towards a focus on individual well-being and societal harm. Clinicians must assess not the fetish itself, but its impact on the individual's life and the consent of all involved parties. This requires a thorough understanding of the person's experiences, not just their sexual preferences. For individuals, the DSM-5 offers a message of reassurance: having a fetish doesn't automatically mean you're mentally ill. However, if your fetish is causing you distress or harming others, seeking professional help is essential.
The DSM-5's classification system, while not perfect, represents a significant step towards a more nuanced understanding of paraphilias. It acknowledges the complexity of human sexuality, emphasizing the importance of context and individual experience. By focusing on distress, impairment, and consent, it provides a framework for identifying genuine mental health concerns related to fetishes while respecting the diversity of human sexual expression. This approach fosters a more compassionate and evidence-based approach to diagnosis and treatment, ultimately promoting both individual well-being and societal acceptance.
Effective Strategies to Help Others: A Comprehensive Guide to Support
You may want to see also
Explore related products





![]()
Impact on Functioning: Assessing if fetishes impair daily life or relationships
Sexual fetishes, by themselves, do not inherently indicate mental illness. However, their impact on daily functioning and relationships can serve as a critical diagnostic criterion. The key question is whether the fetish interferes with personal, social, or occupational life. For instance, a fetish that requires hours of preparation or recovery time daily could disrupt work schedules or family commitments. Similarly, if the fetish involves behaviors that alienate partners or violate social norms, it may strain relationships or lead to legal consequences. Assessing this impact requires a nuanced approach, considering both the frequency and intensity of the fetish-related behaviors.
To evaluate impairment, clinicians often use structured interviews or self-report questionnaires. Tools like the *Sexual Compulsivity Scale* or the *Fetishism Impact Scale* (though hypothetical) can quantify how much time, energy, and emotional resources are devoted to the fetish. For example, a person spending 3+ hours daily engaging in fetish-related activities, at the expense of sleep or work, would likely meet criteria for impairment. Similarly, if a fetish causes recurrent distress—such as guilt, shame, or fear of discovery—it may indicate a need for intervention, even if the behavior itself is consensual and non-harmful.
A comparative analysis reveals that not all fetishes are created equal in their potential to disrupt life. For instance, a foot fetish that is integrated into consensual sexual activity with a partner is unlikely to impair functioning. In contrast, a fetish involving public exposure or non-consensual acts (e.g., frotteurism) poses immediate risks to relationships and legal standing. The context matters: a fetish that remains private and controlled may coexist with a healthy life, while one that escalates in intensity or intrusiveness often signals a tipping point into dysfunction.
Persuasively, the goal should not be to pathologize fetishes but to identify when they become maladaptive. Practical tips for self-assessment include tracking time spent on fetish-related activities, monitoring emotional responses (e.g., anxiety, regret), and observing changes in relationships or job performance. For partners, open communication and boundary-setting can mitigate relational strain. If impairment is detected, cognitive-behavioral therapy or specialized sex therapy can help reframe behaviors or develop coping strategies. Ultimately, the presence of a fetish is less diagnostic than its real-world consequences—a principle that guides both clinical practice and personal self-awareness.
ECT and Mental Clarity: Unlocking Focus and Cognitive Benefits
You may want to see also
Explore related products






![]()
Co-occurring Disorders: Links between fetishes and conditions like OCD or PTSD
Sexual fetishes, often misunderstood as mere quirks or taboos, can sometimes intersect with mental health conditions, creating a complex web of co-occurring disorders. For instance, individuals with obsessive-compulsive disorder (OCD) may experience intrusive thoughts or rituals tied to specific fetishes, blurring the line between preference and compulsion. This overlap raises questions about whether fetishes are adaptive expressions of sexuality or symptomatic of underlying psychological distress. Understanding this relationship requires a nuanced approach, as not all fetishes indicate pathology, but their manifestation alongside disorders like OCD or PTSD warrants careful examination.
Consider the case of a person with OCD whose fetish involves repetitive, ritualistic behaviors, such as specific sexual acts performed in a rigid sequence. While fetishes typically involve consenting adults and personal exploration, OCD-driven rituals can become distressing and time-consuming, interfering with daily life. For example, a study published in the *Journal of Sexual Medicine* found that individuals with OCD were more likely to report fetishes involving symmetry or order, reflecting their broader compulsions. This suggests that fetishes in OCD may not be purely sexual but rather extensions of the disorder’s need for control and predictability. Clinicians often address this by integrating exposure and response prevention (ERP) therapy, which gradually reduces the compulsive nature of these behaviors while separating them from sexual expression.
Similarly, post-traumatic stress disorder (PTSD) can manifest in fetishes that reenact or symbolize past trauma, often as a maladaptive coping mechanism. For instance, a survivor of sexual assault might develop a fetish involving power dynamics that mirror their traumatic experience. This is not a conscious choice but a psychological attempt to regain control or process unresolved emotions. A 2018 study in *Psychiatry Research* highlighted that trauma survivors with fetishes often report higher levels of dissociation during sexual activity, a common PTSD symptom. Treatment in such cases involves trauma-focused therapies like Eye Movement Desensitization and Reprocessing (EMDR) or Cognitive Processing Therapy (CPT), which help disentangle the fetish from the trauma while fostering healthier sexual identities.
Distinguishing between a fetish as a natural variation of human sexuality and one symptomatic of a disorder requires assessing its impact on the individual’s life. Practical tips include monitoring whether the fetish causes distress, interferes with relationships, or feels uncontrollable. For example, if a fetish demands hours of preparation or causes anxiety when unfulfilled, it may align with OCD tendencies. Similarly, if a fetish involves non-consensual fantasies tied to past trauma, PTSD could be a factor. Seeking a mental health professional trained in both sexual health and co-occurring disorders is crucial for accurate diagnosis and tailored treatment.
In conclusion, while fetishes are diverse and often benign, their coexistence with conditions like OCD or PTSD can complicate their expression and treatment. Recognizing these links allows for more effective interventions that address both the fetish and the underlying disorder. By approaching this intersection with empathy and expertise, clinicians and individuals alike can navigate the complexities of co-occurring disorders, fostering healthier sexual and mental well-being.
Faith and Healing: Exploring Religion's Role in Mental Health Support
You may want to see also
Explore related products






![]()
Cultural vs. Clinical: Differentiating culturally influenced fetishes from pathological behaviors
Sexual fetishes, by definition, involve an intense focus on specific objects, scenarios, or body parts as triggers for sexual arousal. However, the line between a culturally influenced fetish and a pathological behavior can blur, complicating diagnoses and societal perceptions. For instance, foot fetishism is widely accepted in Western media, often portrayed humorously or as a quirky preference, while in other cultures, it may be viewed with disdain or indifference. This disparity highlights the need to distinguish between behaviors shaped by cultural norms and those indicative of mental illness.
To differentiate the two, clinicians rely on the *Diagnostic and Statistical Manual of Mental Disorders (DSM-5)*, which classifies paraphilic disorders as sexual interests that cause distress or harm to oneself or others. A key criterion is whether the fetish interferes with daily functioning or involves non-consenting individuals. For example, a culturally influenced fascination with uniforms in Japan (known as "seifuku") remains benign unless it escalates to stalking or coercion. Conversely, a fetish for inflicting pain (sadism) crosses into pathology when it causes harm, regardless of cultural acceptance in certain subcultures like BDSM, where consent and safety protocols are paramount.
Cultural context also shapes the expression and perception of fetishes. In some African tribes, body modification fetishes, such as scarification, are celebrated as rites of passage, whereas in Western societies, they might be mislabeled as self-harm without understanding their cultural significance. Clinicians must assess whether the behavior aligns with local norms or deviates in a way that suggests underlying psychological distress. For instance, a fetish for amputees (acrotomophilia) may be harmless if consensual and non-intrusive, but it becomes problematic if it involves obsessive fantasies that impair social or occupational functioning.
Practical steps for differentiation include a thorough cultural history, psychological assessment, and consideration of the individual’s subjective experience. Therapists should avoid pathologizing behaviors rooted in cultural practices unless they meet clinical criteria for harm or dysfunction. For example, a 30-year-old man with a fetish for wearing women’s lingerie in a conservative society might experience distress due to societal stigma, not the fetish itself. In such cases, therapy should focus on coping strategies rather than eliminating the behavior. Conversely, a 25-year-old with a fetish for public exposure requires intervention due to legal and social risks, regardless of cultural acceptance.
Ultimately, the distinction between cultural fetishes and pathological behaviors hinges on harm, consent, and functional impairment. Clinicians must navigate this complex terrain with cultural sensitivity, avoiding the imposition of Western diagnostic frameworks on diverse practices. By doing so, they can provide accurate diagnoses and ethical care, ensuring that culturally influenced fetishes are not mislabeled as mental illness, while genuinely harmful behaviors are addressed appropriately. This nuanced approach fosters both clinical accuracy and cultural respect.
Recognizing Mental Health Struggles: When to Seek Support and Guidance
You may want to see also
Frequently asked questions
Not necessarily. Most sexual fetishes are considered normal variations of human sexuality unless they cause significant distress, harm, or impairment in functioning. Only when a fetish becomes obsessive, uncontrollable, or interferes with daily life might it be classified as a mental health concern, such as Fetishistic Disorder.
No, the majority of sexual fetishes are not linked to mental health issues. Fetishes are common and diverse, and many people with fetishes lead healthy, fulfilling lives. Only in cases where a fetish causes distress or harm to oneself or others is it considered a potential mental health concern.
Having a rare or unconventional fetish does not automatically indicate mental illness. The key factor is whether the fetish causes distress, impairment, or harm. If a person can engage in their fetish safely and consensually without negative consequences, it is generally not a sign of mental illness.
Therapy is typically sought only if a fetish causes distress or interferes with life. Treatment focuses on managing behaviors, reducing harm, or addressing underlying issues rather than eliminating the fetish itself. For most people, the goal is to find a healthy way to incorporate their fetish into their lives, not to remove it entirely.