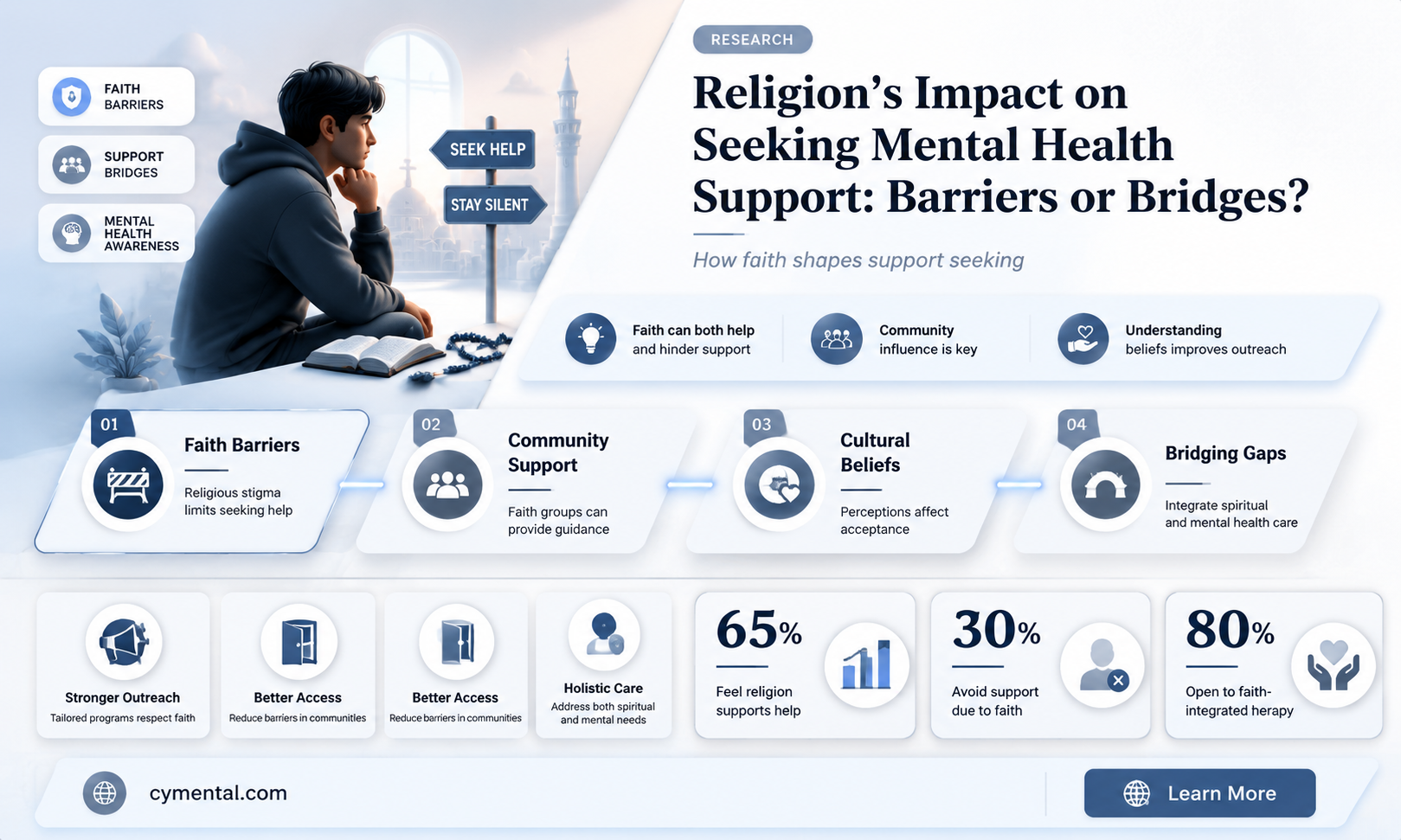
The relationship between religion and mental health treatment is a complex and multifaceted issue, as religious beliefs and practices can significantly influence an individual's willingness to seek professional help. On one hand, religion often provides a sense of community, purpose, and coping mechanisms that can alleviate mental distress, potentially reducing the perceived need for external intervention. However, certain religious doctrines or cultural stigma may discourage followers from pursuing psychological or psychiatric care, viewing mental health issues as a matter of faith, personal weakness, or even spiritual punishment. This interplay raises important questions about how religious identity shapes access to and acceptance of mental health services, highlighting the need for culturally sensitive approaches that bridge the gap between spiritual and clinical support systems.
| Characteristics | Values |
|---|---|
| Prevalence of Mental Health Stigma | Religious communities often hold stigmatizing attitudes towards mental illness, viewing it as a sign of weakness, sin, or lack of faith. This stigma can deter individuals from seeking professional help. |
| Preference for Religious Coping | Many religious individuals prefer seeking support from religious leaders or prayer groups rather than mental health professionals, believing spiritual solutions are sufficient. |
| Conflict with Religious Beliefs | Some religious teachings may conflict with certain mental health treatments (e.g., medication, therapy modalities), leading individuals to avoid or delay seeking help. |
| Lack of Mental Health Education | Religious communities may lack awareness about mental health issues and available resources, hindering access to care. |
| Positive Influence on Help-Seeking | Certain religious beliefs can encourage help-seeking by promoting self-care, compassion, and community support. Some religious leaders actively advocate for mental health awareness. |
| Access to Religious-Based Mental Health Services | The existence of faith-based counseling or integrated care models can increase access to mental health services for religious individuals. |
| Cultural and Demographic Factors | The impact of religion on help-seeking varies across cultures, denominations, and individual beliefs. |
| Need for Culturally Sensitive Care | Mental health professionals need to be culturally competent and respectful of religious beliefs to effectively engage religious individuals in treatment. |
Explore related products





What You'll Learn
- Stigma in religious communities hindering mental health treatment-seeking behavior
- Religious beliefs conflicting with professional psychological interventions and therapies
- Faith-based coping mechanisms as alternatives to clinical mental health care
- Clergy vs. therapists: Role overlap and referral patterns in mental health
- Cultural barriers in religious groups limiting access to mental health services
![]()
Stigma in religious communities hindering mental health treatment-seeking behavior
Religious communities often foster a sense of belonging and support, yet they can inadvertently become barriers to mental health treatment. Stigma surrounding mental illness within these groups frequently stems from misconceptions that equate psychological struggles with weakness, sin, or lack of faith. For instance, in some Christian denominations, depression may be dismissed as a failure to trust God’s plan, while in certain Islamic communities, anxiety might be attributed to insufficient prayer or spiritual devotion. Such beliefs discourage individuals from seeking professional help, fearing judgment or ostracization.
Consider the case of a 28-year-old woman in a conservative evangelical church who delays therapy for her panic attacks because her pastor suggests her symptoms are "spiritual warfare" requiring prayer, not medication. This scenario illustrates how religious leaders, though well-intentioned, may lack the training to distinguish between spiritual crises and clinical mental health conditions. Their influence can inadvertently reinforce stigma, leaving congregants trapped between their faith and their need for evidence-based care.
To address this, religious communities must integrate mental health education into their teachings. For example, faith leaders could collaborate with mental health professionals to host workshops debunking myths like "mental illness is a punishment from God." Practical steps include providing resource lists of faith-sensitive therapists or incorporating mental health testimonials into sermons to normalize seeking help. Parents in these communities should also be encouraged to model openness about mental health, ensuring children feel safe discussing their struggles without fear of spiritual condemnation.
However, caution is necessary when blending faith and mental health. Encouraging prayer or spiritual practices as *complementary* to, rather than replacements for, professional treatment is critical. For instance, a study found that 40% of religiously affiliated individuals who relied solely on prayer for depression experienced worsening symptoms over six months. Balancing spiritual support with clinical intervention requires clear communication and respect for both domains.
Ultimately, dismantling stigma in religious communities demands a dual approach: educating faith leaders to recognize mental health issues and empowering congregants to advocate for themselves. By fostering an environment where faith and mental health care coexist, these communities can transform from obstacles into allies in the journey toward healing. Practical tools, like anonymous support groups within churches or mosques, can bridge the gap, ensuring individuals receive both spiritual solace and clinical treatment without shame.
Melodies of Healing: Music's Powerful Impact on Mental Well-Being
You may want to see also
Explore related products


$19.95 $19.95


$21.49 $32.99


![]()
Religious beliefs conflicting with professional psychological interventions and therapies
Religious beliefs can significantly shape an individual’s willingness to seek or accept professional psychological help, often creating a tension between faith-based practices and evidence-based therapies. For instance, some religious communities view mental health struggles as a test of faith or a result of spiritual weakness, discouraging members from pursuing secular interventions like cognitive-behavioral therapy (CBT) or medication. A 2019 study published in the *Journal of Clinical Psychology* found that 40% of participants from highly religious backgrounds reported feeling conflicted about using antidepressants, believing prayer or spiritual counseling should suffice. This conflict can delay treatment, exacerbating conditions like depression or anxiety, which often require timely, multifaceted approaches.
Consider the case of a 28-year-old woman diagnosed with generalized anxiety disorder whose pastor advised her to "pray harder" instead of seeing a therapist. Despite worsening symptoms, she avoided professional help for over a year, fearing it would contradict her faith. Such scenarios highlight the need for mental health professionals to engage with religious clients in culturally sensitive ways. For example, integrating faith into therapy—such as incorporating prayer into mindfulness exercises or framing CBT techniques as aligning with spiritual growth—can bridge the gap between religious beliefs and psychological interventions. This approach, known as spiritually integrated psychotherapy, has shown promise in improving treatment adherence among religious populations.
However, not all religious beliefs are inherently at odds with mental health care. Some faith traditions actively encourage seeking professional help, viewing it as a complement to spiritual practices. For instance, the Catholic Church has publicly supported mental health treatment, stating that therapy and medication are not incompatible with faith. Yet, even in these cases, specific therapies may conflict with religious values. For example, exposure therapy for OCD might clash with religious scrupulosity, where intrusive thoughts involve religious themes. Therapists must navigate these nuances carefully, ensuring interventions respect the client’s beliefs while addressing clinical needs.
Practical steps can mitigate conflicts between religion and therapy. First, mental health providers should assess clients’ religious beliefs early in treatment, using tools like the Religious and Spiritual Identity Scale (RSI). Second, collaboration with religious leaders can foster trust and reduce stigma. For instance, a therapist might consult a pastor to reinforce the idea that seeking help is an act of stewardship over one’s health. Third, tailoring interventions to align with religious values—such as reframing mindfulness as a form of contemplative prayer—can enhance acceptance. Caution is advised, however, against imposing religious elements on non-religious clients or oversimplifying complex theological concerns.
Ultimately, the goal is not to alter religious beliefs but to create a therapeutic alliance that respects them while prioritizing mental well-being. For example, a therapist working with a devout Muslim client experiencing PTSD might incorporate Quranic verses into trauma-focused therapy, providing comfort while addressing symptoms. Such culturally adaptive approaches require training and humility from providers but can significantly improve outcomes. By acknowledging the role of faith in clients’ lives, mental health professionals can transform potential conflicts into opportunities for holistic healing.
The Right to Refuse: Mental Health Treatment and Autonomy
You may want to see also
Explore related products






![]()
Faith-based coping mechanisms as alternatives to clinical mental health care
For many individuals, faith serves as a cornerstone of emotional resilience, offering coping mechanisms that can rival or complement clinical mental health care. Religious practices such as prayer, meditation, and communal worship provide structured routines that foster a sense of purpose and belonging. For example, a study published in the *Journal of Religion and Health* found that regular prayer was associated with lower levels of anxiety and depression in older adults. These practices often act as preventive measures, helping individuals manage stress before it escalates into a mental health crisis. However, the effectiveness of faith-based coping depends heavily on the individual’s belief system and the supportiveness of their religious community.
Consider the role of faith communities as informal support networks. Churches, mosques, and temples often provide pastoral counseling, support groups, and charitable assistance, filling gaps left by underfunded or inaccessible mental health systems. In low-income regions or areas with limited mental health resources, these faith-based initiatives can be lifelines. For instance, faith leaders in rural communities are increasingly trained to identify signs of mental distress and refer individuals to professional care when needed. Yet, this approach is not without risks. Misguided advice or stigmatizing attitudes within religious groups can deter individuals from seeking evidence-based treatment, highlighting the need for collaboration between faith leaders and mental health professionals.
Faith-based coping mechanisms also leverage spiritual beliefs to reframe suffering, offering narratives of hope and redemption that can be profoundly therapeutic. For someone grappling with depression, viewing their struggle as part of a divine plan or a test of faith can provide meaning and resilience. However, this reframing must be handled delicately. A rigid or punitive interpretation of faith—such as attributing mental illness to sin or lack of faith—can exacerbate distress. Mental health professionals working with religious clients often emphasize the importance of validating spiritual beliefs while encouraging evidence-based interventions like cognitive-behavioral therapy (CBT) or medication when necessary.
Practical integration of faith-based and clinical approaches requires clear boundaries and mutual respect. For example, a therapist might incorporate mindfulness techniques rooted in Buddhist traditions or encourage clients to explore spiritual texts as part of their healing process. Conversely, faith leaders can educate their congregations about mental health, debunking myths and promoting professional care. A collaborative model, such as the one developed by the American Psychological Association’s *Psychology of Religion and Spirituality* division, provides guidelines for integrating spiritual practices into mental health treatment plans. This dual approach acknowledges the strengths of both systems while addressing their limitations.
Ultimately, faith-based coping mechanisms are not a one-size-fits-all solution but a valuable tool for those who find meaning in spiritual practices. Their effectiveness lies in their ability to provide comfort, community, and a sense of purpose—elements often missing in purely clinical interventions. However, individuals and practitioners must remain vigilant against the potential pitfalls of over-reliance on faith alone. By fostering dialogue between religious and mental health communities, we can create a more holistic and inclusive approach to mental well-being, ensuring that no one is left to navigate their struggles in isolation.
Breaking the Silence: Why Men Resist Seeking Mental Health Support
You may want to see also
Explore related products






![]()
Clergy vs. therapists: Role overlap and referral patterns in mental health
In many communities, clergy members are often the first point of contact for individuals seeking help with mental health issues, sometimes even before therapists. This phenomenon raises questions about the role overlap between clergy and mental health professionals and how referral patterns impact access to appropriate care. For instance, a study published in the *Journal of Pastoral Care & Counseling* found that 80% of congregants initially approached their clergy for emotional distress before considering a therapist. This statistic underscores the critical role clergy play in mental health, but it also highlights potential gaps in specialized care.
Consider the case of a 35-year-old woman experiencing anxiety and depression. She confides in her pastor, who offers spiritual guidance and prayer. While this may provide temporary relief, the pastor lacks the training to diagnose or treat her condition effectively. If the clergy member fails to refer her to a therapist, her symptoms could worsen. This scenario illustrates the importance of clear referral pathways. Clergy should be equipped with resources to identify when a situation requires professional intervention and know how to connect individuals with licensed therapists. For example, providing a list of local mental health providers or offering to make a joint call to a therapist’s office can bridge the gap between spiritual and clinical care.
From a comparative perspective, clergy and therapists serve distinct yet complementary roles. Clergy often address existential and spiritual concerns, offering comfort and meaning in times of distress. Therapists, on the other hand, focus on evidence-based interventions to treat mental health disorders. However, the lines blur when clergy attempt to provide therapeutic advice without proper training. For instance, a clergy member might misinterpret symptoms of bipolar disorder as spiritual warfare, delaying appropriate treatment. To avoid such pitfalls, clergy should undergo basic mental health training, such as Mental Health First Aid, which teaches them to recognize symptoms and refer individuals to professionals.
Persuasively, it’s essential to acknowledge the cultural and religious barriers that may prevent individuals from seeking therapy. In some communities, mental health stigma is deeply rooted in religious beliefs, with struggles seen as a lack of faith rather than a medical issue. Clergy can play a pivotal role in destigmatizing mental health by openly discussing its importance from the pulpit and integrating mental health resources into church programs. For example, hosting workshops on stress management or inviting therapists to speak at church events can normalize seeking help. By fostering a culture of acceptance, clergy can encourage congregants to access the care they need.
Practically, establishing formal referral partnerships between religious institutions and mental health providers can streamline access to care. Churches could create a referral network with local therapists who understand the congregation’s cultural and spiritual values. Additionally, clergy should be mindful of their limitations and avoid overstepping into therapeutic territory. For instance, instead of offering advice on managing PTSD, a clergy member could say, “I’m here to support you spiritually, but I also recommend speaking with a therapist who specializes in trauma.” This approach ensures individuals receive holistic care that addresses both their spiritual and mental health needs.
In conclusion, while clergy and therapists serve different roles, their collaboration is crucial for effective mental health care. By understanding their unique contributions, establishing clear referral patterns, and addressing cultural barriers, they can work together to ensure individuals receive the comprehensive support they need. Clergy should view themselves as gatekeepers to mental health services, guiding congregants toward professional help while continuing to provide spiritual solace. This dual approach maximizes the strengths of both roles, ultimately improving mental health outcomes in faith-based communities.
Shooting Survivors: Access to Mental Health Support and Recovery
You may want to see also
Explore related products

$10.99 $16.95





![]()
Cultural barriers in religious groups limiting access to mental health services
Religious communities often prioritize spiritual healing over clinical intervention, creating a cultural barrier that limits access to mental health services. For instance, in some Christian denominations, prayer and faith are seen as the primary tools for overcoming mental distress, with professional therapy viewed as a lack of trust in God’s plan. This belief can deter individuals from seeking help, even when symptoms of anxiety or depression become debilitating. Similarly, in certain Islamic traditions, mental health issues may be attributed to spiritual weakness or possession, leading families to consult religious leaders instead of psychiatrists. Such practices, while rooted in faith, can delay or prevent evidence-based treatment, exacerbating conditions that require timely professional care.
Consider the steps religious groups can take to bridge this gap. First, educate community leaders about the coexistence of faith and mental health care. Workshops or seminars led by mental health professionals can dispel myths and provide practical tools for identifying symptoms. Second, integrate mental health screenings into existing religious programs, such as youth groups or elder care services. For example, a church could partner with a local clinic to offer free depression screenings during community events. Third, encourage the use of faith-sensitive therapy models, like those incorporating scripture or spiritual practices, to make treatment more culturally acceptable. These steps require collaboration but can foster trust and increase service utilization.
A comparative analysis reveals that cultural barriers are not uniform across religious groups. In Orthodox Jewish communities, for instance, the stigma surrounding mental illness often stems from concerns about reputation and marriageability, leading families to avoid diagnosis altogether. In contrast, some Hindu communities may view mental health struggles as the result of past-life karma, emphasizing acceptance over intervention. These differences highlight the need for tailored approaches. A one-size-fits-all strategy fails to address the nuanced beliefs and practices of each group. Mental health advocates must engage with religious leaders to understand these specifics and co-create solutions that respect cultural values while promoting well-being.
Persuasively, it’s critical to address the ethical implications of these barriers. Denying or delaying mental health care due to religious beliefs can lead to severe consequences, including self-harm or chronic disability. While religious freedom is a fundamental right, it should not override an individual’s right to health. Policymakers and healthcare providers must advocate for culturally competent care that respects faith while ensuring access to proven treatments. For example, training therapists to incorporate religious language or practices can make therapy more palatable for devout individuals. Ultimately, the goal is not to challenge religious beliefs but to harmonize them with the imperative of mental health care.
Practically, individuals within religious groups can take proactive steps to navigate these barriers. Start by researching faith-based mental health resources, such as Christian counseling services or Muslim mental health organizations, which blend spirituality with clinical expertise. If resistance arises from family or clergy, frame mental health care as an act of self-preservation, aligning it with religious teachings on stewardship of the body. For parents, model openness by discussing mental health openly with children, reducing stigma early. Finally, advocate for change within your community by sharing personal stories or inviting mental health professionals to speak at religious gatherings. Small, consistent efforts can gradually shift cultural norms and improve access to care.
ADHD Music: A Mental Fatigue Remedy or Myth?
You may want to see also
Frequently asked questions
Yes, religion can influence a person's willingness to seek mental health treatment. Some individuals may turn to religious practices or leaders for support instead of professional mental health services, while others may integrate both. Cultural and religious beliefs about mental health can either encourage or discourage seeking help.
In some cases, religious beliefs can hinder access to mental health care if they stigmatize mental illness or view it as a spiritual failing rather than a medical condition. However, many religious communities are increasingly supportive of mental health treatment and encourage members to seek professional help.
Studies show mixed results. Some research suggests that religious individuals may experience better mental health due to social support and coping mechanisms provided by their faith. Others indicate that religious stigma or guilt can worsen mental health outcomes. It largely depends on the individual's beliefs and their religious community's attitudes.
Religion can sometimes be a barrier if individuals or their communities reject evidence-based treatments in favor of solely spiritual or faith-based interventions. However, many mental health professionals work to integrate religious beliefs into treatment plans to make care more accessible and culturally sensitive.
Mental health professionals can improve treatment outcomes by acknowledging and respecting a client's religious beliefs, incorporating spiritual practices into therapy when appropriate, and collaborating with religious leaders or communities. Building trust and understanding can help clients feel more comfortable seeking and engaging in treatment.



















