Mental health challenges among teenagers have reached alarming levels, yet a significant portion of affected youth are not receiving the necessary support. Studies indicate that a startling percentage of teens struggling with mental illness, such as anxiety, depression, or other disorders, are not accessing professional help due to barriers like stigma, lack of awareness, limited resources, or fear of judgment. This gap in care not only exacerbates individual suffering but also poses long-term risks to their overall well-being and development. Understanding the scope of this issue is crucial to addressing the systemic failures and societal attitudes that prevent vulnerable teens from getting the assistance they desperately need.
| Characteristics | Values |
|---|---|
| Percentage of teens with mental illness | Approximately 20% (ages 13-18) experience a severe mental disorder |
| Percentage not receiving treatment | 50-70% of teens with mental health issues do not receive treatment |
| Reasons for lack of treatment | Stigma, lack of access, cost, and unawareness of symptoms |
| Gender disparities | Females are more likely to seek help than males |
| Racial/ethnic disparities | Minority teens face greater barriers to accessing mental health care |
| Impact of untreated mental illness | Increased risk of academic failure, substance abuse, and suicide |
| Availability of school-based services | Only 20% of schools have adequate mental health resources |
| Parental awareness | 1 in 5 parents underestimate the severity of their child's symptoms |
| Telehealth usage | Increased during the pandemic but still underutilized |
| Global perspective | Similar trends observed in high-income countries, worse in low-income |
Explore related products


$6.53 $12.99


What You'll Learn
- Barriers to Access: Financial constraints, lack of awareness, and stigma prevent teens from seeking mental health support
- Underdiagnosis Rates: Many teens go undiagnosed due to overlapping symptoms and limited screening in schools
- Cultural Factors: Cultural beliefs and language barriers discourage teens from discussing mental health issues
- Fear of Stigma: Teens avoid help due to fear of judgment, bullying, or being labeled as weak
- Lack of Resources: Insufficient mental health services in rural or underserved areas leave teens unsupported
![]()
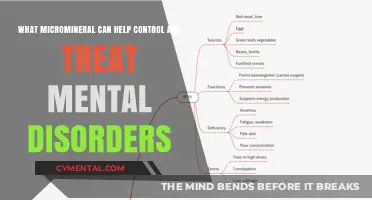
Barriers to Access: Financial constraints, lack of awareness, and stigma prevent teens from seeking mental health support
A staggering 60% of adolescents with mental health disorders receive no treatment, according to the National Institute of Mental Health. This alarming statistic highlights a critical issue: teens are struggling in silence, often due to barriers that prevent them from accessing the support they desperately need. Among these barriers, financial constraints, lack of awareness, and stigma stand out as significant roadblocks.
Consider the financial burden of mental health care. Therapy sessions can range from $65 to $250 per hour, and psychiatric evaluations may cost upwards of $500. For families without insurance or with high deductibles, these expenses are prohibitive. Even with insurance, copays and limited coverage for specialized treatments like dialectical behavior therapy (DBT) or cognitive behavioral therapy (CBT) can leave families struggling to afford consistent care. Teens from low-income households are particularly vulnerable, as they often lack the resources to navigate these financial hurdles, leaving them without access to essential services.
Lack of awareness compounds this issue. Many teens and their families are unaware of the signs of mental illness or the resources available to them. For instance, symptoms like persistent sadness, sudden changes in behavior, or withdrawal from social activities are often dismissed as "typical teenage behavior." Schools, which could serve as critical touchpoints for early intervention, frequently lack trained staff to identify and address these issues. Without proper education and outreach, teens may not recognize their struggles as treatable conditions, delaying or preventing them from seeking help.
Stigma remains one of the most insidious barriers. Fear of judgment or labeling often keeps teens from opening up about their mental health. Phrases like "just snap out of it" or "you’re too young to be depressed" perpetuate the misconception that mental illness is a sign of weakness or a phase. This stigma is particularly harmful in communities where mental health is viewed as taboo, leaving teens isolated and reluctant to seek support. Even when resources are available, the fear of being ostracized can deter teens from taking the first step toward recovery.
To dismantle these barriers, a multi-faceted approach is necessary. Schools and communities must prioritize mental health education, teaching teens and their families to recognize symptoms and understand the importance of early intervention. Policymakers should work to expand insurance coverage for mental health services, ensuring that cost is not a barrier to care. Finally, public campaigns aimed at reducing stigma can encourage open conversations about mental health, fostering an environment where teens feel safe seeking help. By addressing these barriers head-on, we can ensure that fewer teens slip through the cracks and more receive the support they need to thrive.
Cooking for Calm: How Kitchen Therapy Boosts Mental Well-Being
You may want to see also
Explore related products

$13.48 $15.97
$9.59 $16.99



![]()
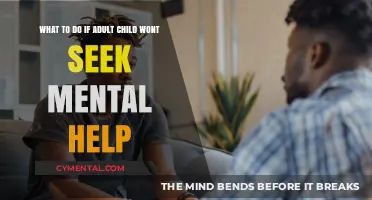
Underdiagnosis Rates: Many teens go undiagnosed due to overlapping symptoms and limited screening in schools
A staggering 50% of all lifetime mental illness begins by age 14, yet studies show that up to 70% of teens with mental health conditions don’t receive the treatment they need. This alarming gap isn’t just a statistic—it’s a crisis fueled by underdiagnosis. One major culprit? Overlapping symptoms that blur the lines between typical teenage behavior and serious mental health issues. Anxiety, for instance, can masquerade as shyness or academic stress, while depression often hides behind irritability or mood swings. Without clear, distinct markers, even vigilant parents and educators may miss the signs, leaving teens to struggle silently.
Schools, where teens spend a significant portion of their day, are ideally positioned to identify mental health issues early. Yet, most lack systematic screening programs. Only 20% of U.S. schools conduct mental health screenings, and even then, these assessments are often rudimentary or optional. Without standardized tools like the Columbia Suicide Severity Rating Scale or the Strengths and Difficulties Questionnaire, red flags slip through the cracks. Compounding this issue is the shortage of school counselors: the national average is 1 counselor per 422 students, far exceeding the recommended 1:250 ratio. Overworked staff simply can’t provide the individualized attention needed to spot subtle symptoms.
Consider ADHD and anxiety, two conditions that frequently overlap in teens. Both can cause restlessness, difficulty concentrating, and avoidance of social situations. A teen with undiagnosed ADHD might be labeled as "lazy" or "unmotivated," while one with anxiety might be dismissed as "overly sensitive." Without a comprehensive evaluation, these teens may never receive the targeted interventions—like cognitive-behavioral therapy or stimulant medications—that could transform their lives. Similarly, bipolar disorder in teens often presents as extreme mood swings, which can be mistaken for hormonal fluctuations typical of adolescence. This misattribution delays diagnosis by an average of 10 years, during which untreated symptoms can worsen.
To bridge this gap, schools must adopt universal mental health screenings as part of routine wellness checks, starting in middle school. Tools like the PHQ-9 for depression or GAD-7 for anxiety can be administered annually, with results flagged for follow-up by trained professionals. Parents can also play a proactive role by tracking behavioral changes over time—for example, noting if a teen’s sleep patterns shift dramatically or if their grades drop without an obvious cause. If three or more symptoms (e.g., persistent sadness, withdrawal from activities, unexplained physical complaints) persist for two weeks, it’s time to consult a pediatrician or mental health specialist. Early intervention isn’t just beneficial—it’s critical, as untreated mental illness in teens increases the risk of academic failure, substance abuse, and suicidal ideation by 50%.
The takeaway? Underdiagnosis isn’t inevitable. By recognizing the complexity of overlapping symptoms and advocating for robust screening in schools, we can ensure that teens receive the support they need before their struggles escalate. It’s not about overmedicalizing adolescence but about equipping young people with the tools to thrive. After all, mental health isn’t a luxury—it’s a fundamental right, and one that’s far too often denied to those who need it most.
Supporting Your 34-Week Baby's Mental Growth: Essential Tips and Strategies
You may want to see also
Explore related products





![]()
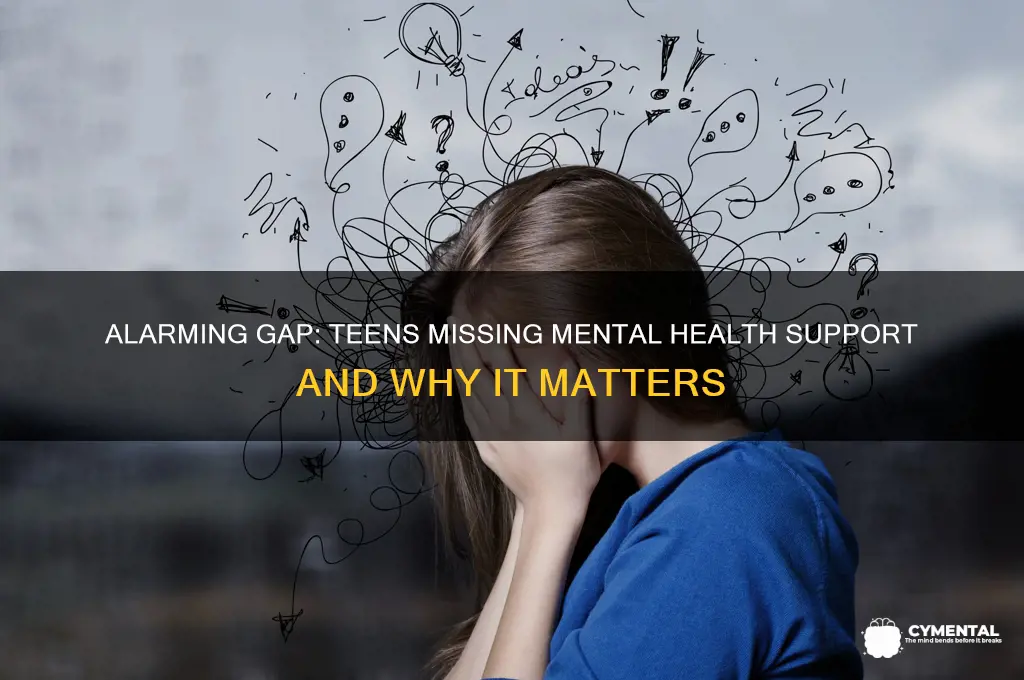
Cultural Factors: Cultural beliefs and language barriers discourage teens from discussing mental health issues
Cultural stigma surrounding mental health is a significant barrier for teens seeking help, particularly in communities where emotional struggles are seen as a sign of weakness or family shame. In many Asian and Hispanic cultures, for instance, mental illness is often attributed to personal failure or spiritual imbalance rather than a treatable condition. A 2021 study published in the *Journal of Adolescent Health* found that 60% of Asian American teens reported feeling pressured by family to hide mental health issues to avoid bringing dishonor. This internalized stigma creates a silence that prevents teens from even acknowledging their struggles, let alone seeking professional intervention.
Language barriers compound this issue, especially for immigrant teens or those in multilingual households. Mental health terminology is often abstract and culturally specific, making it difficult to translate accurately. For example, the concept of "depression" may not exist in the same form in some languages, leading to misunderstandings or minimization of symptoms. A 2019 report by the National Alliance on Mental Illness (NAMI) highlighted that only 17% of mental health providers in the U.S. are bilingual, leaving many teens without access to care in their native language. This lack of linguistic accessibility reinforces feelings of isolation and discourages teens from reaching out.
Consider the case of a 16-year-old Latina teen whose parents equate therapy with "locura" (craziness). Despite experiencing severe anxiety, she avoids mentioning her symptoms at home, fearing her parents will dismiss her as ungrateful or dramatic. At school, her limited English proficiency prevents her from articulating her struggles to counselors, who mistakenly attribute her withdrawal to cultural shyness. This double bind—cultural stigma at home and linguistic barriers at school—leaves her trapped in a cycle of untreated mental illness. Her story is not unique; it reflects the experiences of countless teens whose cultural and linguistic realities shut them out of the mental health system.
To address these barriers, schools and healthcare providers must adopt culturally responsive practices. For instance, hiring bilingual mental health professionals or offering translated resources can bridge the language gap. Community-based programs that involve parents and elders in mental health education can help dismantle stigma by framing mental wellness as a collective responsibility rather than an individual flaw. For example, a pilot program in California used storytelling workshops to engage Latino families in conversations about mental health, resulting in a 30% increase in teens seeking counseling services. Such initiatives demonstrate that cultural sensitivity, paired with practical solutions, can create pathways to care for marginalized teens.
Ultimately, the intersection of cultural beliefs and language barriers is a systemic issue that requires systemic solutions. Until mental health services are designed with cultural humility and linguistic inclusivity, teens from diverse backgrounds will continue to fall through the cracks. The goal is not to erase cultural differences but to ensure they do not become obstacles to care. By acknowledging and addressing these factors, we can move closer to a reality where every teen, regardless of their background, feels empowered to seek the help they need.
Occupational Therapy: Empowering Mental Health Recovery and Daily Functioning
You may want to see also
Explore related products





![]()
Fear of Stigma: Teens avoid help due to fear of judgment, bullying, or being labeled as weak
A staggering 60% of adolescents experiencing mental health issues do not seek professional help, according to recent studies. This alarming statistic highlights a pervasive issue: the fear of stigma. For many teens, the prospect of being judged, bullied, or labeled as weak is a powerful deterrent to reaching out for support. This fear is not unfounded; societal attitudes and peer dynamics often reinforce the notion that seeking help is a sign of failure or inadequacy.
Consider the classroom setting, where a teenager might overhear peers mocking someone for "overreacting" or "being too sensitive." Such casual dismissals of emotional struggles create an environment where vulnerability is perceived as a liability. For instance, a 15-year-old with anxiety might avoid school counseling services because they fear being ostracized by their friends. This avoidance is not merely a personal choice but a response to a culture that often equates mental health struggles with personal flaws.
To address this, schools and communities must actively dismantle the stigma surrounding mental health. One practical step is to integrate mental health education into curricula, normalizing conversations about emotions and struggles. For example, workshops that teach students how to recognize signs of mental health issues in themselves and others can foster empathy and reduce judgment. Additionally, anonymous support systems, such as online chat services or peer-led groups, can provide teens with a safe space to seek help without fear of exposure.
Parents and caregivers also play a critical role in mitigating stigma. Encouraging open dialogue about mental health at home can help teens feel more comfortable seeking help. For instance, a parent might share their own experiences with stress or anxiety, modeling vulnerability and resilience. It’s essential to emphasize that seeking help is a sign of strength, not weakness, and to reinforce this message consistently.
Ultimately, breaking the cycle of stigma requires collective effort. By challenging harmful stereotypes, providing safe avenues for support, and fostering a culture of empathy, we can empower teens to prioritize their mental well-being without fear of judgment. The goal is not just to reduce the percentage of teens avoiding help but to create a society where seeking support is seen as a normal and courageous act.
Logic's Role in Managing Mental Illness: A Thoughtful Exploration
You may want to see also
Explore related products






![]()
Lack of Resources: Insufficient mental health services in rural or underserved areas leave teens unsupported
In rural America, nearly 70% of counties lack a single psychiatrist, leaving teens with limited access to mental health care. This stark statistic highlights a critical issue: geographic isolation often translates to isolation from essential services. For adolescents in these areas, the nearest mental health provider might be hours away, making regular therapy sessions or emergency interventions nearly impossible. The digital divide further exacerbates the problem, as telehealth options—while increasingly popular—require reliable internet access, a luxury not all rural communities enjoy.
Consider the logistical hurdles: a 16-year-old in a small Montana town, struggling with anxiety, might need to travel 100 miles to see a therapist. Even if transportation is available, the time and cost involved can deter families from seeking help. Schools, often the first line of defense in identifying mental health issues, may lack counselors or social workers trained to address these needs. Without local resources, teens are left to navigate their struggles alone, increasing the risk of untreated conditions escalating into crises.
The disparity in mental health resources between urban and rural areas is not just a matter of convenience—it’s a matter of equity. Urban teens have access to walk-in clinics, specialized programs, and peer support groups, while their rural counterparts often rely on overburdened primary care physicians who may lack the expertise to treat complex mental health issues. For example, a study found that rural teens are 50% less likely to receive mental health treatment compared to their urban peers. This gap widens when considering marginalized groups, such as LGBTQ+ teens or those from low-income families, who face additional barriers to care.
To address this crisis, policymakers and healthcare providers must prioritize innovative solutions. Mobile clinics, for instance, can bring mental health services directly to underserved communities. Schools can integrate mental health education into curricula and train staff to recognize warning signs. Telehealth programs, paired with efforts to expand rural broadband access, could bridge the gap for teens in remote areas. Additionally, incentivizing mental health professionals to practice in rural regions—through loan forgiveness or salary supplements—could increase the availability of local providers.
Ultimately, the lack of mental health resources in rural and underserved areas is a solvable problem, but it requires targeted action. By investing in infrastructure, technology, and workforce development, we can ensure that no teen is left unsupported simply because of where they live. The cost of inaction—measured in untreated illnesses, lost potential, and preventable tragedies—is far greater than the investment needed to create equitable access to care.
Supporting Your Daughter's Mental Health: A Guide for Concerned Parents
You may want to see also
Frequently asked questions
Studies indicate that approximately 60% of teens with mental health issues do not receive any form of treatment or professional help.
Common barriers include stigma surrounding mental health, lack of access to affordable care, insufficient awareness of symptoms, and fear of judgment from peers or family.
Increasing mental health education in schools, expanding telehealth services, reducing costs, and promoting open conversations about mental health can help more teens receive the support they need.