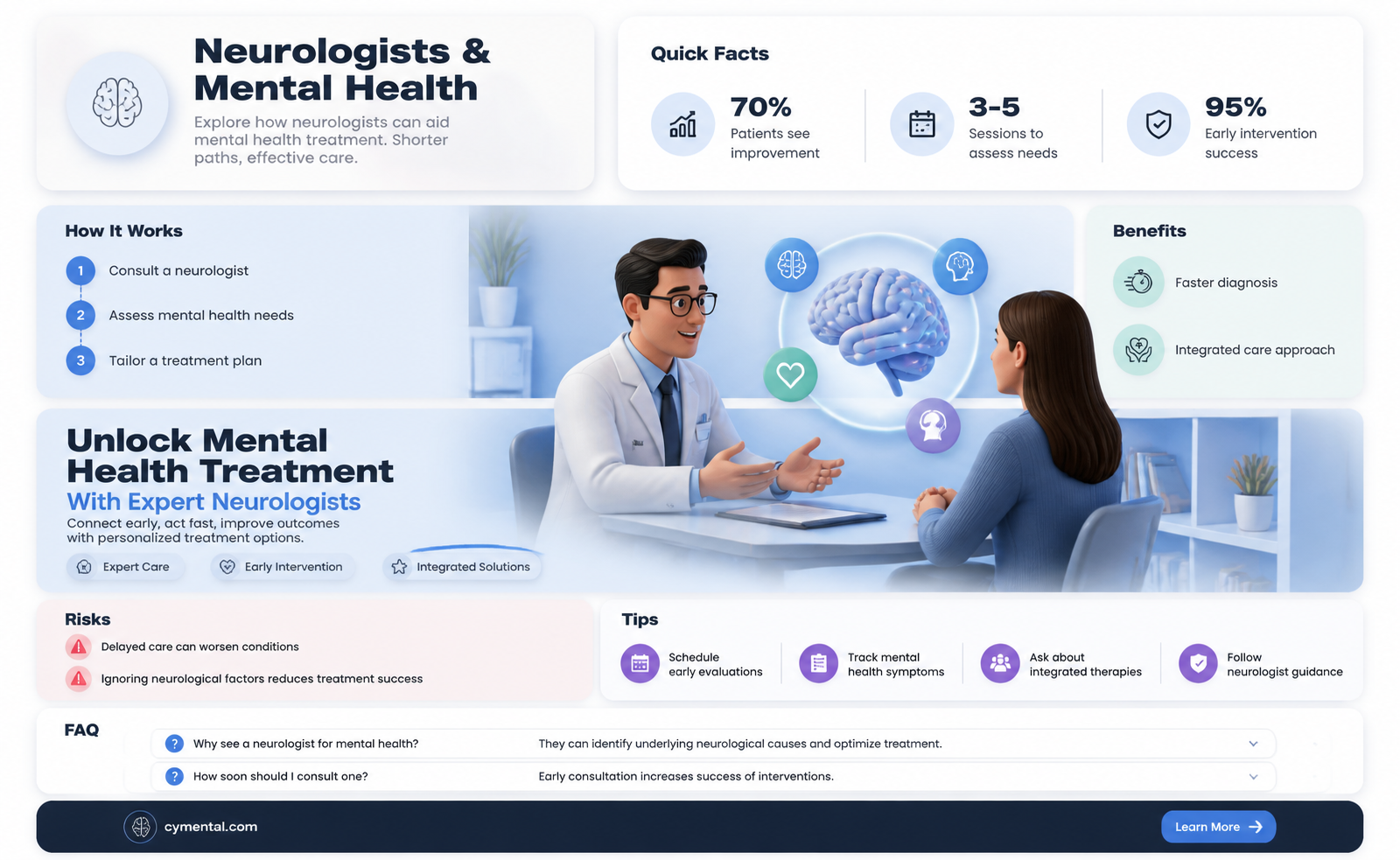
Neurologists, traditionally focused on disorders of the nervous system such as epilepsy, stroke, and multiple sclerosis, are increasingly being recognized for their potential role in addressing mental illness. While psychiatrists are typically the primary providers for mental health conditions, there is growing evidence of the intricate link between neurological function and mental health. Conditions like depression, anxiety, and bipolar disorder often have neurological underpinnings, such as imbalances in neurotransmitters or structural brain changes. Neurologists, with their expertise in brain physiology and advanced diagnostic tools like EEGs and MRIs, can offer unique insights into these conditions, particularly when they co-occur with neurological disorders or when symptoms are treatment-resistant. However, their involvement is often complementary to psychiatric care, highlighting the need for an integrated approach to treating the complex interplay between the brain and mind.
| Characteristics | Values |
|---|---|
| Role of Neurologists | Neurologists specialize in disorders of the nervous system, including the brain, spinal cord, and nerves. They primarily diagnose and treat neurological conditions like epilepsy, stroke, multiple sclerosis, and Parkinson’s disease. |
| Overlap with Mental Illness | Some mental health conditions have neurological underpinnings (e.g., depression linked to brain structure changes, ADHD with neurological components). Neurologists may identify or rule out neurological causes of psychiatric symptoms. |
| Collaboration with Psychiatrists | Neurologists often work with psychiatrists to differentiate between neurological and psychiatric disorders, especially in cases like psychosis, mood disorders, or cognitive decline. |
| Treatment Contributions | Neurologists may prescribe medications (e.g., anticonvulsants for mood stabilization) or recommend treatments like transcranial magnetic stimulation (TMS) or neurofeedback for conditions with neurological overlap. |
| Limitations | Neurologists are not primary mental health providers. They do not offer psychotherapy or specialized psychiatric care. Mental illnesses are typically managed by psychiatrists, psychologists, or therapists. |
| Conditions Where Neurologists Help | - Neuropsychiatric disorders (e.g., Tourette syndrome, obsessive-compulsive disorder with tic disorders). - Cognitive impairment or dementia. - Traumatic brain injury with psychiatric sequelae. - Epilepsy-related mood or behavioral changes. |
| Latest Research | Emerging studies highlight the neurobiological basis of mental illnesses, encouraging interdisciplinary approaches. Neurologists contribute to research on brain circuitry and neuroinflammation in conditions like schizophrenia and depression. |
| Patient Referral | Patients with complex symptoms (e.g., hallucinations, cognitive decline) may be referred to neurologists to exclude neurological causes before psychiatric treatment. |
| Preventive Care | Neurologists may address lifestyle factors (e.g., sleep, diet) that impact both neurological and mental health. |
| Technological Advances | Use of neuroimaging (MRI, fMRI) and EEG by neurologists aids in understanding brain function in mental health disorders. |
Explore related products





What You'll Learn
- Neurological vs. Psychiatric Disorders: Overlapping Symptoms and Treatments
- Neuropsychiatric Conditions: When Neurology and Psychiatry Intersect
- Brain Imaging: Neurologists’ Role in Diagnosing Mental Health Issues
- Neurological Treatments for Mental Illness: TMS, DBS, and More
- Referral Criteria: When to Consult a Neurologist for Mental Health
![]()
Neurological vs. Psychiatric Disorders: Overlapping Symptoms and Treatments
Neurological and psychiatric disorders often present with overlapping symptoms, blurring the lines between brain function and mental health. For instance, a patient experiencing memory loss might be diagnosed with depression, a side effect of certain medications, or early-stage dementia—each requiring vastly different treatments. This complexity underscores the need for a nuanced approach to diagnosis and care, where neurologists and psychiatrists may collaborate to untangle the root causes of symptoms.
Consider the case of seizures, a neurological phenomenon, which can mimic psychiatric conditions like panic attacks or psychosis. A neurologist might prescribe antiepileptic drugs such as levetiracetam (500–1,500 mg twice daily) to control seizures, while a psychiatrist could recommend cognitive-behavioral therapy to address anxiety. Conversely, conditions like Parkinson’s disease often come with psychiatric symptoms—depression, anxiety, or hallucinations—requiring a dual treatment strategy. Here, a neurologist might adjust dopamine agonists, while a psychiatrist introduces selective serotonin reuptake inhibitors (SSRIs) like sertraline (50–200 mg daily) to manage mood disorders.
The interplay between these fields is further evident in conditions like multiple sclerosis (MS), where fatigue, cognitive impairment, and mood disturbances are common. Neurologists focus on disease-modifying therapies (e.g., interferon beta-1a, 22–44 mcg subcutaneously three times weekly), while psychiatrists address depression or anxiety with psychotherapy and medications. Practical tips for patients include maintaining a symptom journal to track physical and emotional changes, which can aid both specialists in tailoring treatment plans.
A persuasive argument emerges for integrated care models, where neurologists and psychiatrists work in tandem. For example, in treating traumatic brain injury (TBI), neurologists manage physical sequelae, while psychiatrists address post-traumatic stress disorder (PTSD) or mood disorders. This collaborative approach ensures holistic care, reducing the risk of misdiagnosis or incomplete treatment. Patients, particularly those over 65 or with complex histories, benefit from such coordination, as age-related changes can exacerbate both neurological and psychiatric symptoms.
In conclusion, the overlap between neurological and psychiatric disorders demands a multidisciplinary strategy. By recognizing shared symptoms and leveraging complementary treatments, healthcare providers can deliver more effective care. Patients should advocate for comprehensive evaluations and seek providers willing to collaborate, ensuring no aspect of their health is overlooked. This approach not only improves outcomes but also fosters a more accurate understanding of the intricate relationship between brain and mind.
Yoga's Transformative Power: Enhancing Mental Health and Well-being Naturally
You may want to see also
Explore related products






![]()
Neuropsychiatric Conditions: When Neurology and Psychiatry Intersect
Neuropsychiatric conditions blur the lines between brain function and mental health, demanding a collaborative approach that transcends traditional medical silos. These disorders, such as epilepsy with psychosis, Parkinson’s disease with depression, or Alzheimer’s disease with agitation, manifest symptoms that intertwine neurological and psychiatric domains. For instance, a patient with temporal lobe epilepsy may experience seizures alongside hallucinations or mood disturbances, requiring expertise from both neurology and psychiatry. This intersection highlights the need for integrated care, as these conditions often share underlying neurobiological mechanisms, such as dysregulated neurotransmitter systems or inflammatory pathways.
Consider the case of a 52-year-old woman diagnosed with Parkinson’s disease who develops severe treatment-resistant depression. Her neurologist adjusts her dopamine agonists, but her symptoms persist. A psychiatrist steps in, prescribing a selective serotonin reuptake inhibitor (SSRI) at a starting dose of 20 mg daily, titrated up to 40 mg over four weeks. Simultaneously, the neurologist recommends cognitive-behavioral therapy tailored to Parkinson’s patients. This dual approach addresses both the neurological basis of her motor symptoms and the psychiatric dimension of her depression, illustrating how interdisciplinary care can optimize outcomes.
The diagnostic process for neuropsychiatric conditions is equally complex. Take autoimmune encephalitis, where patients present with acute psychosis, memory loss, or seizures. A neurologist might order an MRI and lumbar puncture to detect antibodies like NMDA-R, while a psychiatrist evaluates for primary psychotic disorders. Misdiagnosis is common without this collaborative lens, as psychiatric symptoms often overshadow the underlying neurological cause. For example, a 28-year-old man with anti-NMDA-R encephalitis was initially treated for schizophrenia until neurological intervention revealed the autoimmune etiology, leading to immunotherapy with corticosteroids and intravenous immunoglobulin (IVIG).
Practical tips for patients and caregivers navigating neuropsychiatric conditions include maintaining open communication between specialists, tracking symptoms in a journal to identify patterns, and advocating for comprehensive testing. For instance, if a patient with multiple sclerosis develops anxiety, caregivers should ensure the neurologist and psychiatrist coordinate care, as anxiety may stem from disease progression, medication side effects, or psychological distress. Additionally, lifestyle modifications, such as regular exercise and a Mediterranean diet, can support both neurological and psychiatric health, though these should complement, not replace, medical treatment.
In conclusion, neuropsychiatric conditions demand a paradigm shift from fragmented care to integrated models. By recognizing the shared biological and clinical features of these disorders, neurologists and psychiatrists can collaborate to deliver more precise, effective treatments. Patients benefit from this synergy, as it addresses the full spectrum of their symptoms, improving quality of life and functional outcomes. This intersection is not just a theoretical concept but a practical necessity in modern medicine.
Overcoming Mental Blocks: Strategies to Support Athletes' Performance and Resilience
You may want to see also
Explore related products






![]()
Brain Imaging: Neurologists’ Role in Diagnosing Mental Health Issues
Neurologists, traditionally associated with conditions like epilepsy and stroke, are increasingly leveraging brain imaging to diagnose and differentiate mental health disorders. Advanced techniques such as functional MRI (fMRI), positron emission tomography (PET), and diffusion tensor imaging (DTI) allow them to map neural activity, metabolic patterns, and structural connectivity. For instance, fMRI can identify hyperactivity in the amygdala in patients with anxiety disorders, while PET scans reveal reduced glucose metabolism in the prefrontal cortex of individuals with depression. These objective biomarkers complement clinical assessments, reducing reliance on subjective symptom reporting.
Consider a 35-year-old patient presenting with severe mood swings and cognitive fog. A psychiatrist might diagnose bipolar disorder based on behavioral symptoms, but a neurologist could order a DTI scan to assess white matter integrity. If the scan shows abnormalities in the anterior cingulate cortex—a region critical for emotional regulation—this structural insight could refine the diagnosis and treatment plan. For example, transcranial magnetic stimulation (TMS) might be recommended to target this specific area, offering a more precise intervention than standard pharmacotherapy.
However, integrating brain imaging into mental health diagnosis isn’t without challenges. False positives and negatives are common, as many psychiatric disorders share overlapping neural signatures. For instance, both ADHD and schizophrenia can show prefrontal cortex hypoactivity on fMRI. Additionally, the cost and accessibility of these technologies limit their widespread use. A single PET scan can cost $3,000–$5,000, and interpreting results requires specialized training. Neurologists must therefore balance the benefits of imaging with practical considerations, often reserving it for complex or treatment-resistant cases.
To maximize the utility of brain imaging, neurologists collaborate with psychiatrists and psychologists in a multidisciplinary approach. For example, a patient with treatment-resistant depression might undergo a PET scan to measure serotonin transporter density, guiding the selection of SSRIs or alternative therapies like ketamine infusions. This team-based strategy ensures that imaging data is contextualized within the patient’s broader clinical picture, avoiding over-reliance on scans while harnessing their diagnostic potential.
In practice, patients and clinicians alike should view brain imaging as a tool, not a panacea. While it provides valuable insights into the neurobiology of mental illness, it cannot replace the nuanced understanding gained from patient history and behavioral observation. For instance, a teenager with suspected OCD might show basal ganglia hyperactivity on fMRI, but the severity and impact of their compulsions still require detailed clinical evaluation. By combining imaging with traditional methods, neurologists can offer more personalized, evidence-based care in the complex landscape of mental health.
Supporting the Mentally Handicapped: Are Current Efforts Truly Making a Difference?
You may want to see also
Explore related products


$91.99 $150




![]()
Neurological Treatments for Mental Illness: TMS, DBS, and More
Neurologists are increasingly playing a pivotal role in treating mental illness, leveraging advanced neurological interventions that target the brain’s circuitry. Among these, Transcranial Magnetic Stimulation (TMS) and Deep Brain Stimulation (DBS) stand out as groundbreaking therapies. TMS, a non-invasive procedure, uses magnetic fields to stimulate specific brain regions associated with mood regulation, such as the prefrontal cortex. Approved by the FDA for treatment-resistant depression, TMS typically involves 20–30 sessions over 4–6 weeks, with each session lasting 20–40 minutes. Patients remain awake and alert, experiencing minimal side effects like mild headaches or scalp discomfort. DBS, on the other hand, is an invasive procedure where electrodes are implanted into precise brain areas, delivering electrical impulses to modulate abnormal neural activity. While primarily used for Parkinson’s disease, DBS has shown promise in severe cases of obsessive-compulsive disorder (OCD) and treatment-resistant depression, though it remains experimental for broader psychiatric use.
The efficacy of TMS and DBS highlights the brain’s plasticity and its potential for rewiring in mental health treatment. TMS, for instance, has a response rate of approximately 50–60% in patients with major depressive disorder who have failed prior antidepressants. Its success lies in its ability to normalize hyperactive or hypoactive brain regions without systemic side effects, making it a viable option for those intolerant to medications. DBS, while more invasive, offers profound benefits for select patients, with studies showing significant symptom reduction in 60–70% of OCD cases. However, its high cost, surgical risks, and need for long-term management limit its accessibility. Both treatments underscore the importance of personalized medicine, as their effectiveness varies based on individual brain anatomy and illness severity.
Beyond TMS and DBS, emerging neurological treatments like Vagus Nerve Stimulation (VNS) and Focused Ultrasound (FUS) are expanding the therapeutic landscape. VNS, initially used for epilepsy, involves implanting a device that stimulates the vagus nerve, which connects to mood-regulating brain regions. It has shown modest but consistent benefits for treatment-resistant depression, with improvements often appearing after several months. FUS, a non-invasive technique using ultrasound waves, is being explored to modulate deep brain structures without surgery, though its psychiatric applications remain in early clinical trials. These innovations reflect a shift toward precision psychiatry, where treatments are tailored to the neurobiological underpinnings of mental illness rather than relying solely on trial-and-error pharmacotherapy.
While these neurological treatments offer hope, they are not without limitations. TMS, for example, requires a significant time commitment and may not provide lasting benefits without maintenance sessions. DBS carries risks such as infection, hardware malfunction, and mood changes, necessitating careful patient selection and monitoring. Additionally, the high cost of these therapies often restricts access, raising ethical questions about equity in mental healthcare. Clinicians must weigh these factors against the potential for life-changing improvements, particularly for patients who have exhausted conventional treatments.
In practice, integrating neurological treatments into mental health care requires collaboration between neurologists, psychiatrists, and other specialists. Patients considering TMS or DBS should undergo thorough evaluations, including brain imaging and psychiatric assessments, to determine suitability. For TMS, practical tips include scheduling sessions during low-stress times and maintaining a consistent sleep schedule to enhance efficacy. DBS candidates should be fully informed about the procedure’s risks and long-term commitments, such as regular device checks. As research advances, these treatments may become more refined and accessible, offering new avenues for individuals struggling with refractory mental illness.
Athletes and Mental Health: Why Seeking Help Remains a Challenge
You may want to see also
Explore related products

$140 $200





![]()
Referral Criteria: When to Consult a Neurologist for Mental Health
Neurologists, traditionally associated with conditions like epilepsy or stroke, increasingly play a pivotal role in mental health care. Their expertise in brain function and structure positions them to address cases where psychiatric symptoms may stem from neurological abnormalities. This intersection is particularly relevant when mental health symptoms are refractory to standard treatments or present atypically, suggesting an underlying organic cause.
Consider a 32-year-old woman with treatment-resistant depression and new-onset migraines. Despite trials of three antidepressants and therapy, her mood remains severely impaired. The addition of neurological symptoms like migraines and subjective cognitive decline warrants a neurology referral. Here, the neurologist might investigate for conditions like multiple sclerosis or autoimmune encephalitis, which can mimic psychiatric disorders. This example underscores the importance of recognizing red flags that signal a need for neurological evaluation.
Referral criteria should include persistent or severe symptoms that defy conventional psychiatric explanations. Key indicators are cognitive changes (e.g., sudden memory loss, confusion), movement disorders (e.g., tremors, dystonia), or sensory disturbances (e.g., hallucinations with no psychiatric history). Additionally, patients with a history of traumatic brain injury, seizures, or neurodegenerative diseases require careful monitoring for co-occurring mental health issues. For instance, post-concussion syndrome often includes anxiety and depression, necessitating a neurologist’s input to manage both physical and psychological sequelae.
Practical steps for clinicians include documenting the timeline of symptoms, ruling out substance-induced or medication-related causes, and assessing for neurological deficits during psychiatric evaluations. Collaboration between psychiatrists and neurologists is essential, especially in complex cases. For example, a patient with psychosis and abnormal gait might benefit from an MRI to exclude structural lesions like tumors or vascular abnormalities. Early involvement of a neurologist can prevent misdiagnosis and ensure targeted treatment.
In conclusion, neurologists are invaluable in mental health care when symptoms suggest an organic etiology. By recognizing specific referral criteria—such as treatment resistance, neurological red flags, or comorbid conditions—clinicians can bridge the gap between psychiatry and neurology, improving patient outcomes. This interdisciplinary approach ensures that mental health treatment is comprehensive, addressing both mind and brain.
Sleep's Role in Boosting Mental Health and Emotional Well-Being
You may want to see also
Frequently asked questions
Yes, a neurologist can help with certain mental illnesses, particularly those linked to neurological conditions or brain function, such as depression or anxiety associated with epilepsy, Parkinson’s disease, or traumatic brain injuries.
Neurologists often address mental health issues related to neurological disorders, including mood disorders, cognitive impairment, psychosis, or behavioral changes caused by conditions like multiple sclerosis, stroke, or dementia.
It depends on the cause of your symptoms. If your mental health issues are suspected to be linked to a neurological condition, a neurologist may be appropriate. For primary psychiatric disorders like depression or anxiety, a psychiatrist is typically the best choice.
Yes, neurologists can prescribe medications for mental health symptoms, especially when they are related to neurological conditions. However, for primary psychiatric disorders, a psychiatrist is generally more specialized in managing such medications.